INTRODUCTION
The chin is the most prominent part of the frontal facial outline. Protruding together with the nose, it is an important structure forming the lateral facial outline. When the size, shape, position, and ratio of the chin are harmonized with the other facial parts, a beautiful and balanced facial contour is formed. When asymmetry or dysmorphism of the chin has a major effect on the facial appearance, genioplasty is needed for cosmetic or reconstructive reasons [1]. Among various facial plastic techniques, genioplasty follows relatively simple surgical procedures with highly satisfactory results. Moreover, it has been widely used worldwide.
There have been many advances in genioplasty since Trauner and Obwegeser [2] first introduced the approach via an oral cavity incision. Currently, various genioplastic procedures are being used to correct chin deformities.
Horizontal osteotomy, implant genioplasty, and graft genioplasty are examples of genioplastic procedures [3]. However, these approaches are limited in that they cannot correct abnormal laterality or dimensional deformation using a single operation technique and fail to meet patients' aesthetic requirements for facial appearance from frontal, lateral, and inferior perspectives. Therefore, the importance of a preoperational 3Dimensional analysis of the facial contour needs to be emphasized.
Comparative analysis of clinical photographs and cephalometric analysis have generally been used to evaluate patients before undergoing facioplasty. With new developments in imaging technology, 3-dimensional (3D) imaging has been used clinically, which has led to advances in analyzing and correcting facial contours. The use of 3D computed tomography (CT) has made preoperational 3D analysis possible, with consideration of anteroposterior, left-to-right, and superoinferior relationships.
In the present paper, the authors report cases of successful genioplasty for various chin deformities, with consideration of anteroposterior, left-to-right, and superoinferior relationships, using a single operation technique via T-shaped osteotomy with a 3D CT analysis of the facial contour.
METHODS
Patients
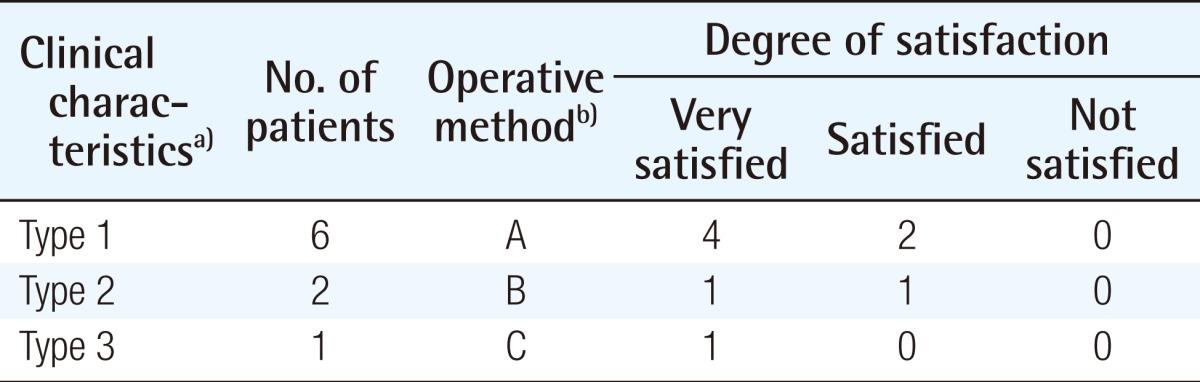
T-shaped genioplasty was performed in 9 patients who visited our hospital between January 2011 and January 2013. The patients were between 18 and 24 years of age, with more women than men (7:2). Of the 9 patients, 6 had macrogenia and 3 had microgenia. In addition, reduction angloplasty was performed in 5 patients with prominent mandibular angles (Table 1).
Surgical techniques
Clinical photographs were taken before the operation to determine the outline of the facial soft tissue. Using facial 3D CT and cephalography, the shape and degree of the chin deformity were determined.
Cephalometric analysis was used in the preoperative analysis to measure the left-to-right asymmetry to the front and anteroposterior asymmetry to the lateral deformity. Moreover, 3D CT provided data regarding the overall facial contour of the 3D difference in left-to-right asymmetry, length ratio of the upper chin to the lower chin, and 3D changes in the lower chin after anteroposterior movement. The 3D preoperative analysis was useful in establishing a surgical plan with consideration of the shape of the chin deformity in macrogenia and microgenia, and the satisfaction of the patients' requirements.
All of the patients underwent the procedure under general anesthesia, and nasal intratracheal intubation was applied to facilitate access to the surgical site. Approaching the surgical site via the oral cavity required injection with 1% lidocaine and 1:100,000 diluted epinephrine solution to the lower gingival sulcus.
Using a periosteal elevator, the space between the mental foramen and periosteum of the inferior part of the mental foramen was exfoliated, and care was taken to conserve the soft tissues in the lower and posterior parts of the chin and not to damage either of the mental nerves.
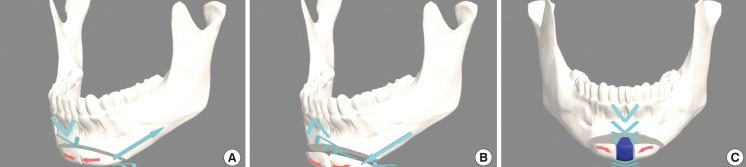
The horizontal line of the osteotomy for genioplasty was drawn 5 mm under the mental foramen so as not to damage the mental nerve, and a vertical line was drawn along the mandible symphysis. The lines were marked, and osteotomy was performed using oscillating and reciprocating saws.
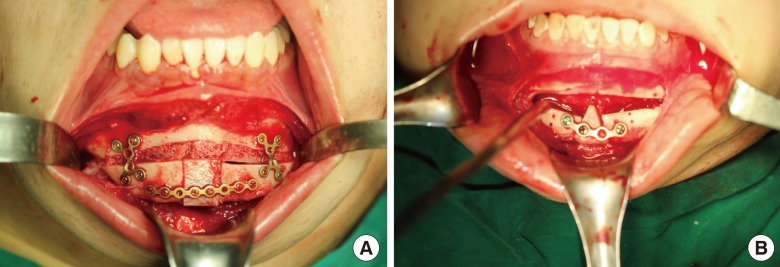
The osteotomed segments were rearranged anteroposteriorly, from left to right, and superoinferiorly, according to the patients' preferences, and the lines of the osteotomy were drawn from the preoperative 3D facial contour (Fig. 1). The osteotomed segments were then fixed with miniplates. According to each patient's chin category, 2 osteotomed segments were subjected to either horizontal shortening or horizontal widening, using bone grafts to induce left-to-right adjustments. Bone fragments were obtained from the iliac bone, or bone pieces after reduction angloplasty were trimmed and used as bone grafts. In addition, to induce upper-to-lower changes, vertical shortening between the mandible and horizontal separated segments and vertical lengthening using bone grafts were performed. This time, bone grafting was performed using the iliac bone or fragmented angle bone to cover the bone gap (Fig. 2). Using the aforementioned methods, left-to-right and upper-to-lower changes were induced; at the same time, segments were moved forward or backward to correct the chin anteroposterior deformity, as determined in the preoperative analysis.
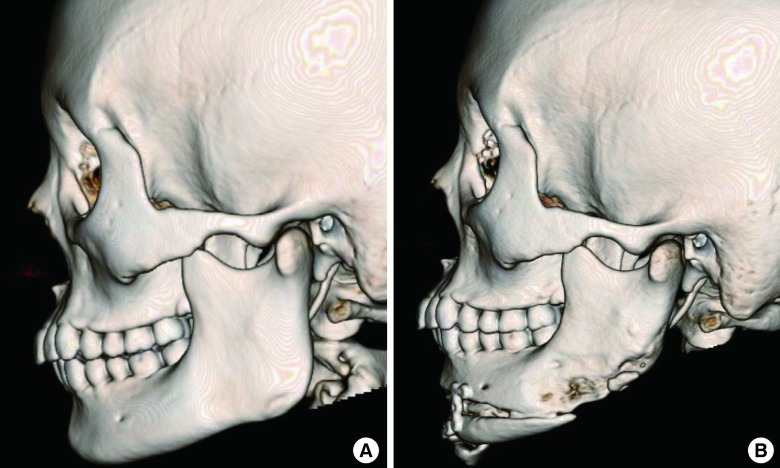
The 3D correction of the chin deformity was confirmed using postoperative photographs and facial 3D CT (Fig. 3). The patients' satisfaction and possible postoperative complications (wound dehiscence, chin hypoesthesia, dysarthria, etc.) were surveyed.
RESULTS
T-shaped genioplasty was performed successfully in all of the cases. No severe complications were observed. Postoperative recovery was uneventful, and all the wounds healed by primary intention without local infection. No facial paralysis or trismus was observed in any of the patients. Transient sensory disturbance of the skin around the mental nerve area was observed in 2 cases, but all of the patients recovered without sequelae within 6 months after the operation.
Case 1
A 19-year-old woman had a chief complaint of prominent chin, requiring correction of the long and projective chin shape. Hence, 2-mm vertical shortening, 5-mm horizontal shortening, and 7-mm backward sliding were performed, and T-shaped genioplasty resulted in a much improved facial profile (Fig. 4).
Case 2
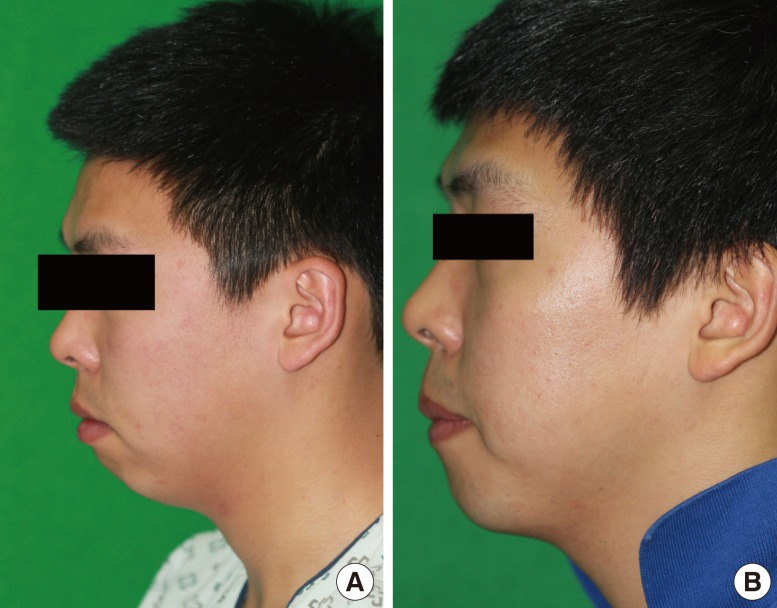
A 22-year-old man had a chief complaint of a short chin and sharp chin shape. An iliac bone graft was used for 3-mm vertical lengthening, 6-mm horizontal widening, and 3-mm forward sliding. T-shaped genioplasty resulted in a much improved facial profile (Fig. 5).
Case 3
An 18-year-old woman had a chief complaint of a short chin and wide square chin, for which reduction angloplasty was performed. A fragmented angle bone was used as a graft for the 9-mm vertical lengthening, and 6-mm horizontal widening was performed. T-shaped genioplasty resulted in a much improved facial profile (Fig. 6).
DISCUSSION
The position and shape of the chin are essential to a beautiful facial contour and are important in determining personal impressions. A small and underdeveloped chin gives a weak, inactive, and passive impression. In contrast, a protruding chin, also called lantern chin, gives a strong and masculine impression. Such chin characteristics can be corrected by a relatively simple genioplastic procedure, which can markedly improve the facial contour. Genioplasty is a widely used cosmetic surgical procedure, as it does not leave superficial scars, with rare adverse effects and high patient satisfaction [4].
Since genioplasty via the oral cavity was introduced by Trauner and Obwegeser [2] in 1957, many advances in surgical technique for chin deformity correction have followed. In 1964, Converse and Wood-Smith [5] presented various approaches to horizontal osteotomy. Recently, diverse corrective procedures for chin deformity, such as the sliding, jumping, graft, and wedge genioplastic techniques, along with narrowing genioplasty, have been performed [6,7].
Among the many types of genioplastic procedures, chin implant insertion is the most common, as it is simple and requires only a short operation time. However, it has been associated with a high risk of infection and complications (implant exposure, implant movement, etc.) [3].
Moreover, genioplasty with implant insertion is limited in that it is not applicable to a severely short chin, protruding chin, asymmetric deformities, or complicated shapes [8].
As a chin deformity is determined based on the relative volume and position of the other facial parts, a regularly shaped implant is not suitable for creating a 3D chin shape.
Other genioplastic procedures such as the sliding, jumping, and graft genioplastic techniques also focus on a single correction point; therefore, they are inadequate for 3D correction given the asymmetric deformity, volume, or position of the chin. Hence, such genioplastic techniques require modification according to characteristics of the chin deformity and patient requirements. In this study, the authors performed T-shaped genioplasty to satisfy the patients' preoperative requirements. Given the 3D chin deformity, anteroposterior, left-to-right, and superoinferior modifications were applied during the operation.
For satisfactory chin deformity correction, understanding patient requirements and the details of the chin deformity are important.
The current preoperative analysis for genioplasty involves a comparison of photographs and a cephalometric analysis. However, with new developments in imaging technology, application of 3D analysis in clinics has become possible and has brought many advances in facial contour analysis and correction. For 3D correction of an asymmetric deformity and for consideration of chin volume and position, the authors actively applied 3D CT in the preoperative and postoperative analyses.
The cephalometric analysis used here allows measurement of the facial contour lines before surgery. However, depending on the completeness of the radiographic results, an inappropriate index could be selected, which could lead to erroneous measurements, making preoperative and postoperative comparisons difficult. Obtaining data from a 2D analysis is also a major limitation of cephalometric analysis. Differing among its various parts, the facial skeleton is assembled with many complicated forms of facial bones. Therefore, a 3D perspective on the facial skeleton is important for any facial operation. Simple radiography or the current 2D CT are not capable of measuring volume, making it difficult to obtain a 3D perspective of a deformity. For example, when performing genioplasty, an anteroposterior deformity and a left-to-right asymmetry could be expected via preoperative analysis; however, adjustment of the position of the osteotomy line or length of movement during the operation is difficult owing to variations in chin thickness.
However, with the development of radiology and computer software, 3D CT images could be constructed from 2D images to make possible the observation of complicated anatomic structures of the craniofacial skeleton. Such 3D CT images can provide a better view of the cutting surface, anatomical positions, and lesions, allowing for more clearly defined spatial relations, to make observations, movements, magnification, and minimization from various angles. These are useful in evaluating lesions and establishing our surgical plans [9,10]. Therefore, genioplasty with personalized T-shaped osteotomy necessarily requires 3D CT. To correct the bone fragments from top to bottom, from left to right, and from front to rear, the predictive analysis of symmetry of the appearance after osteotomy must be performed first. In addition, the characteristics of the contouring between the jaw and the mandibular angle as well as their symmetry must first be understood. To achieve this process, use of 3D CT is necessary.
The authors used such advantages of 3D CT and performed cephalometric analysis and 3D analysis, with preoperative consideration of the anteroposterior, left-to-right, and superoinferior relations in the chin. In brief, the need for mandibular correction and its degree were first determined by preoperative cephalometric analysis, and then 3D asymmetry was analyzed and the method of contouring were planned using 3D CT and 3D modeling tools. Using genioplasty with T-shaped osteotomy, which makes 3D correction possible in a single surgical procedure, the authors were able to obtain satisfactory outcomes.
When compared with the ideal chin shape, the chin in microgenia is located posteriorly when observed from a lateral view. To correct such a deformity, sliding genioplasty is generally performed. The chin could be advanced horizontally; however, vertical elongation is difficult and the vertical length could be shortened in some cases [11]. For microgenia cases, we used preoperative 3D CT to analyze 3D horizontal and vertical movements of the chin and performed T-shaped osteotomy. The osteotomed chin was moved anteroposteriorly, and vertical lengthening was induced. In addition, for correction of a sharp chin due to severe microgenia, horizontal widening was performed, resulting in a satisfactory outcome that met the patient's requirements. The bone gap formed from the horizontal widening and vertical lengthening was filled with an iliac bone graft, and the angle bone fragment formed in the patients who underwent angloplasty was used for a bone graft.
Many cases of macrogenia manifest as a long chin, bent anteriorly when observed from a lateral view. It is important to minimize the length of the chin and at the same time consider its relationship with horizontal protrusion. In our study, we performed T-shaped osteotomy to adjust the vertical upper-to-lower relationship and horizontal lines based on the preoperative 3D CT analysis results. In addition, to satisfy the patients' requirements regarding chin shape, the horizontal width was narrowed. However, in macrogenia, the degree of osteotomy required was predicted given the degree of correction of the horizontal and vertical lines and mandibular angle. An erroneous degree and line of osteotomy may cause microgenic features. Therefore, using preoperative 3D CT, the corrective procedure for the overall lower facial contour was described to the patients before they underwent the procedure.
The T-shaped genioplasty that the authors performed is flexible and suitable for anteroposterior, left-to-right, and superoinferior corrections according to patients' requirements and 3D modifications. Based on the results of the preoperative analysis of the chin deformity and flexibility of the correction, T-shaped osteotomy was the most useful approach.
First, using horizontal osteotomy, corrections of the vertical length and anteroposterior position of the chin were possible. Vertical osteotomy was performed according to mandible symphysis. The width of the incisal surface was narrowed or widened, and the vertical line of osteotomy was moved to correct the left-to-right asymmetry. However, some cases of left-to-right asymmetry could not be corrected despite horizontal and vertical adjustments. In such cases, additional osteotomy in an osteotomed segment was performed to balance both sides.
We were able to the secure anteroposterior, left-to-right, and superoinferior movements of the bone fragments in a 3D manner using T-shaped osteotomy. Based on the results of the preoperative 3D CT analysis, genioplasty was successful in all the patients, fulfilling the patients' requirements and correcting the chin deformity with satisfactory results. However, we were genuinely sorry that our study had severe limitations with regard to cephalometric analysis. Due to its two-dimensional characteristics, this type of analysis still has limitations in identifying the relationship with 3D biological phenomena. Cephalometry is limited, especially in the analysis following 3D correction that this study pursued. A number of studies have recently been conducted on this relationship, but definite relationships among landmarks as well as between 2D cephalometry and cephalometric methods in 3D CT have not yet been established. For further discussion on this matter, cephalometric analyses and landmarks of facial bone contouring surgery using 3D CT should be investigated in the future [12]. With our technique, considering 3D correction preoperatively and postoperatively, a stepladder appearance, which may occur in osteotomed sites, could be minimized and various efficient bone rearrangements could be applied according to patients' requirements.