INTRODUCTION
Bite injuries are becoming more common with the increasing pet population worldwide. The incidence in Europe and the United States is reported to be 175 to 740 bites per 100,000 inhabitants; however, the number of unreported cases is probably much higher [
1]. Mammalian bite wounds most frequently occur on the upper extremities, especially the hands. In addition, some studies have reported a large percentage of bites on the facial area [
1,
2]. The most common mammalian bite injury is inflicted by dogs, accounting for 80% to 90% of all bites, followed by cats and humans [
3]. Management of a bite wound should be sufficiently sophisticated to prevent wound infection, rabies, tetanus, and undue scarring [
4]. However, the optimal management of bite wounds is controversial.
Meanwhile, researchers have performed fragmentary analyses of bite wounds caused by some mammalian species. However, little practical information is available concerning serious mammalian bite wounds that require hospitalization and intensive wound management. Moreover, few studies have been conducted to analyze mammalian bite patients in Korea [
5,
6]. Therefore, the purpose of this study was to perform a general review of cases of mammalian bite wounds requiring inpatient management.
DISCUSSION
Although the incidence of bites has increased to epidemic proportions in recent years, bites are still not recognized as a significant medical problem [
7]. In this study, we analyzed various aspects of mammalian bite wounds and used our findings as bases for recommending guidelines for the care of such cases.
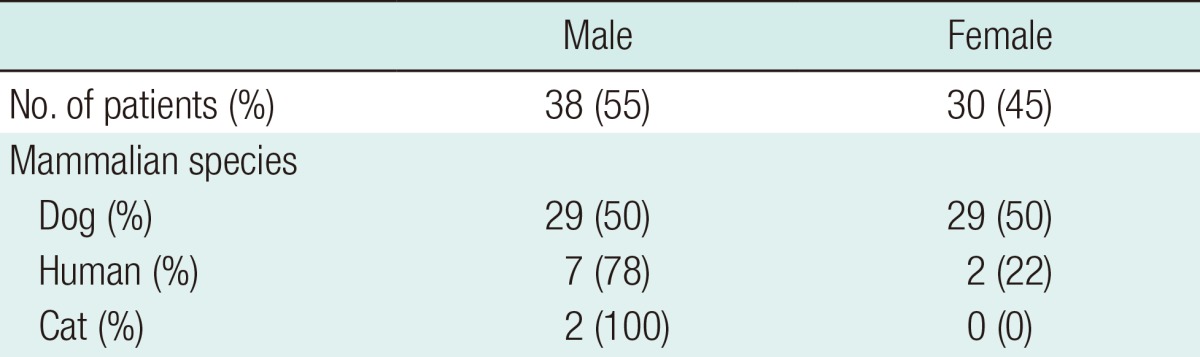
The high incidence of dog bites (85%) in our study is similar to the results of other studies [
8,
9]. However, our findings differ from those of other studies in that human bites were more frequent than cat bites [
3,
10]. The high incidence of human bites in our study was possibly because human bite wounds are frequently related to severe infections or complications that require hospitalization.
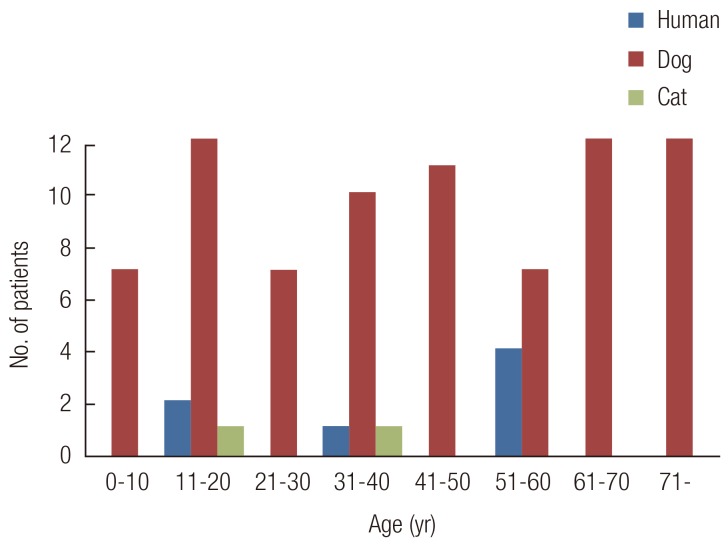
The sex and age distributions in our cases of dog bites differed from those in other studies, which frequently involved men and children [
3,
7,
11,
12]. The finding that a greater number of human bites occurred among men than women is similar to those of other reports [
10,
13]. The propensity for men to be bitten by dogs was considered esplainable by the tendency of men to be more aggressive with dogs [
7]. The similar incidence of dog bites among men and women in our study might have resulted from their similar behaviors toward their dogs, regardless of whether this was during playtime. Meanwhile, the high incidence of human bites among men might have resulted from their aggressive behavior and from the fact that all the cases happened during a fight.
Traditionally, dog bites have been considered a problem among children. However, the patients' ages were randomly distributed in our results. Parents' protective behavior and education of their children may be related to the decreased incidence of dog bites in children.
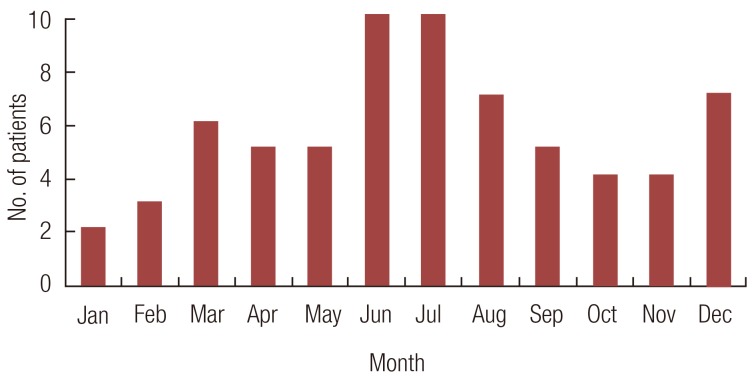
Most studies have indicated that animal bites usually happen during the warmer months [
7]. The seasonal distribution of mammalian bites in this study is similar to that reported previously. The possible reasons for this trend are that less clothing is worn and the outdoor activity of dogs and humans increases during the warm months. The peak incidence of bites in the afternoon and early evening correlates with the time people are most actively engaged with their pets [
7,
11,
14].
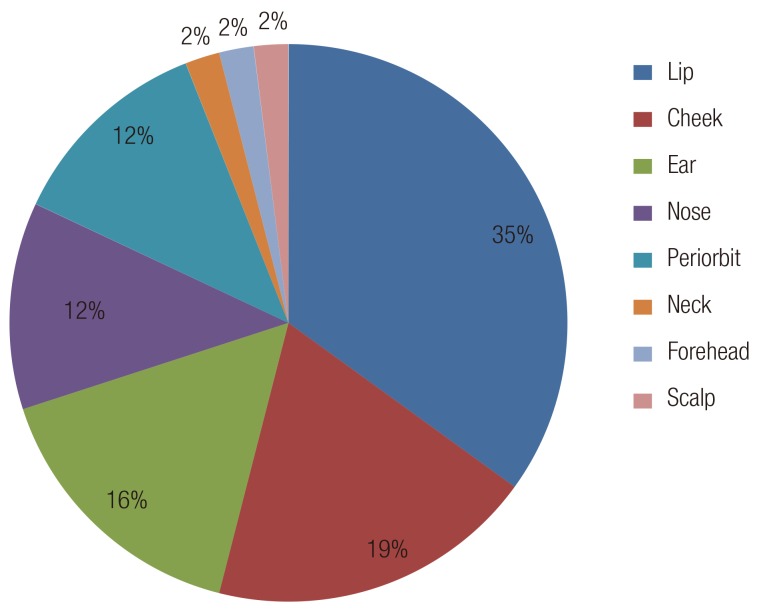
The anatomic distribution of dog bites in this series is different from that in other studies. Many authors have reported that the most frequent site of dog bites is the extremities (54%-85%) [
15,
16]. In this study, however, 62% of the dog bites were located on the facial area. In particular, more than one-third of the dog bites on the face involved the lip area, which is probably caused by being bitten while kissing the dog [
7].
Unlike the cases of dog bites, the anatomic distribution of human and cat bites are consistent with those in previous studies, which indicated that 60% to 67% of cat bites and 60% to 75% of human bites occurred on the upper extremities, particularly the hands and fingers [
17,
18].
Infection is the most common bite-associated complication. In their studies, Maimaris and Quinton [
19], as well as Callaham [
20], demonstrated a correlation between the time of the first medical treatment and the infection rate. In our patients, most of those with delayed initial treatment already showed clinical signs of infection. Culture samples were obtained from the 26 patients (38%) who had signs of clinical infection. However, bacteriological evidence of wound infection was found only in three patients. These cases involved deep, punctiform bite wounds and a cat bite wound in 1 patient. The first case was that of a male patient who developed an abscess caused by
P. multocida growth in a wound on the fourth finger incurred from a cat bite. The abscess was drained and healed with secondary intention a week later. The second case was that of a child who sustained a deep puncture wound to the forearm and developed cellulitis. The bacterial culture was positive for
S. epidermidis, and the infection resolved with delayed direct closure combined with intravenous administration of cephalosporin. The third case was that of a patient who sustained a puncture wound to the first web space of the right hand. The culture was positive for
K. pneumonia. Specific intravenous antibiotics were not replaced in any of the three cases because cephalosporin used prophylactically is sensitive to the three pathogens isolated from the infected wounds. Several clinically infected wounds were found to be sterile by both aerobic and anaerobic culture testing. There are several possible explanations for this result; it may be due to the low diagnostic value of swab cultures or the use of antibiotics and irrigation before obtaining culture samples. This false negative culture phenomenon has also been reported in other studies [
21]. Thus, we focused primarily on the clinical manifestations rather than the culture results.
In our study, the high rate of infection on the hand is similar to that noted by Perron et al. [
22]. As noted previously, clinical and bacteriological evidence of wound infection was found on the hands and forearms in 3 patients. In particular, wounds appearing to be minor injuries often result in serious injury to the extensor tendon or joint capsule and have significant contamination by oral bacteria. The tendon glides upward, thus carrying contaminants with it; therefore, evaluation needs to be performed with the hand in the open and clenched positions. In 2 cases, the extensor tendon of the finger was injured. Before performing repair of the extensor tendon, we controlled the infection by exploration, irrigation, and debridement until there was no evidence of infection. In contrast, the excellent blood supply in the face and the use of prophylactic antibiotics make infection on the facial area a rare occurrence [
23].
The indications for antibiotic prophylaxis depend on the delay between the bite and medical treatment, the animal species, the anatomical structures involved and the extent of the bite. Previous studies have demonstrated no difference in the incidence of infection between the patients given and those not given prophylactic antibiotics [
1,
14,
17]. However, in our patient population, all of the patients received prophylactic antibiotics because most of them had a contaminated wound or severe injury on initial evaluation. The duration of the antibiotic therapy was based on the wound status and treatment response. Administering tetanus prophylaxis for all of the non-immunized patients is also part of the treatment protocol [
12]. It is interesting that half of the human bite patients in our study received a tetanus antitoxin. Lowry reported that this is unnecessary because no case of tetanus bacilli has been isolated in the human mouth, and tetanus has never been reported after a human bite [
23,
24].
Primary closure was not performed either because almost every wound was grossly contaminated or soft tissue injuries were severe. As an initial treatment, local wound cleansing to prevent infection was performed in all of the patients. We irrigated the wounds with iodine solutions and saline, and deep or punctured wounds were additionally cleaned using a syringe with a needle. Surgical debridement was performed in deeper injuries and infected bites. After resolution of inflammatory signs, delayed direct closure, among other delayed treatments, was mostly performed on the patients for aesthetic purposes.
One minor limitation of this study was the small population of patients with cat bite wounds, which might have impeded an accurate analysis of the cases. It must be acknowledged that almost all studies of bite wounds, and therefore this review, are subject to bias because they are based on data from the patients who seek medical attention. Our selected group was more likely to have serious wounds requiring hospitalization. Hence, further studies with a larger population should be conducted. Based on our overall findings from this review of 68 cases of mammalian bites, we recommend the following practical guidelines for the management of mammalian bite injuries requiring in-patient management:
-Early intensive local wound cleansing is the most important therapy for preventing infection.
-Cephalosporin is recommended as the first line empirical antibiotic for patients who require hospitalization.
-After the complete control of infection, a proper reconstruction method has to be considered to achieve aesthetically optimal results.
-On the treatment of facial bite wounds, it is important to build good rapport with the patients and select an aesthetically proper reconstructive method to minimize post-treatment scarring.
-Bites involving the hands have a higher risk of becoming infected. To maximize functional outcomes, initial evaluation and early treatment for controlling infection should be performed.
We believe that these recommendations based on a case review may be useful in the treatment of severe mammalian bite wounds.