Modified vacuum-assisted wound closure with a surgical glove has been proven effective [1]. Fournier's gangrene is a condition that has the possibility of sepsis and delayed healing. Vacuum-assisted wound closure has been done with V.A.C Vacuum-assisted closure (KCI, San Antonio, TX, USA) for scrotal wounds [2,3,4]. We would like to suggest the use of a vacuum with a surgical glove for healing a scrotal wound following Fournier's gangrene. We have found that this method promotes faster healing in a low-cost setting.
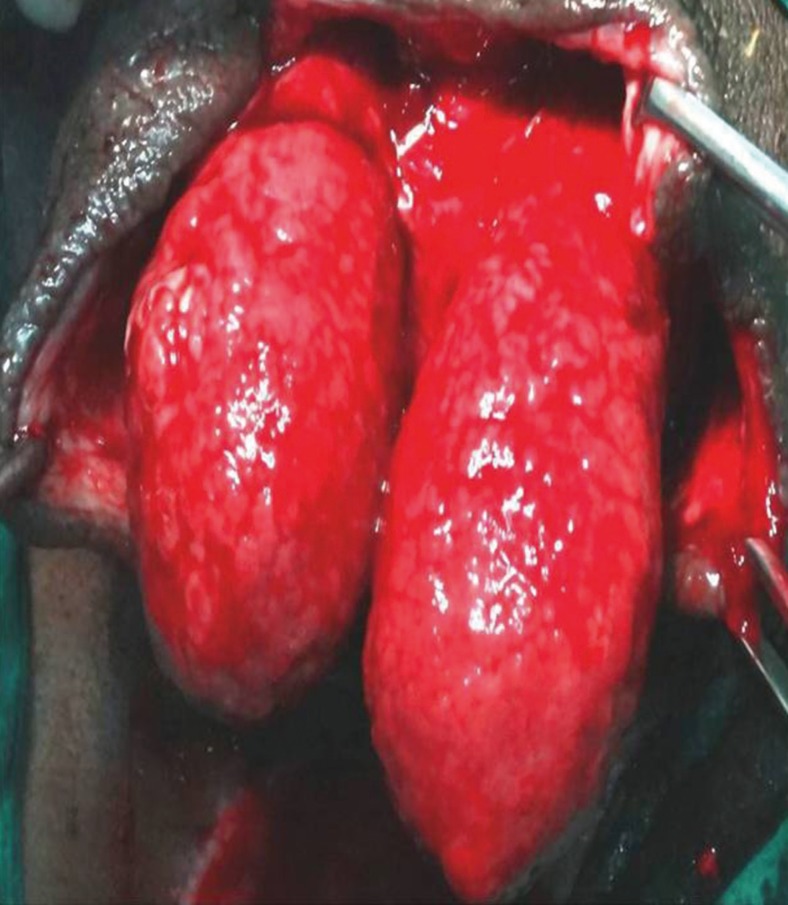
A 46-year-old type-2 diabetes mellitus patient presented with Fournier's gangrene and sepsis syndrome. Following debridement (Fig. 1), modified vacuum dressing was performed with a sterile size 7½ surgical glove. The glove was cut as shown in Fig. 2 and stapled circumferentially at the base beyond the edges of the wound with the other end cut open below the fingers. The interior of the glove was packed with sterile foam or gauze with a suction catheter or Ryle's tubing (Fig. 3). The free end of the glove was plicated and sealed with opsite or with the latex ring of the glove, and a vacuum was created using a suction machine (Fig. 4). An intermittent suction of 125 mm of Hg for 20 min/hr was applied. The tubing and foam was changed every day after a thorough wash by exteriorising the interior of the glove without removing the staples. This method is very similar to the use of a Bogota bag [5]. Consequently, the edema was reduced drastically, and the slough was entirely cleared out of the wound on day 11 following debridement. The wound contracted well, and the patient opted for primary closure on day 16 (Fig. 5). The wound closure was done by raising the scrotal flaps. The postoperative period was uneventful, and the wound healed well.
We suggest that whenever possible for scrotal wounds with a rim of scrotum remaining, modified vacuum dressing can be attempted with a surgical glove, as done in this case. A surgical glove fits snugly to the irregularity of the contour and can be used to apply a vacuum and promote faster healing. It is a sterile, cheap, and effective method. The change of dressing is relatively easy, and the vacuum-assisted closure reduces systemic inflammatory response syndrome, and the duration of hospital stay.