Rice body is an uncommon condition first described in 1895 and associated with tuberculosis tenosynovitis [1]. Resembling rice, the lesion has been called rice body, melon seed, and millet seed, and is encountered as a manifestation of rheumatoid disorders or tuberculosis [1]. In areas where tuberculosis is endemic, rice body tenosynovitis is related to a typical manifestation of extra-pulmonary tuberculosis. Herein, we describe a rare case of rice body tenosynovitis in a hand that showed no evidence of any infections or rheumatic diseases after repetitive diagnostic procedures.
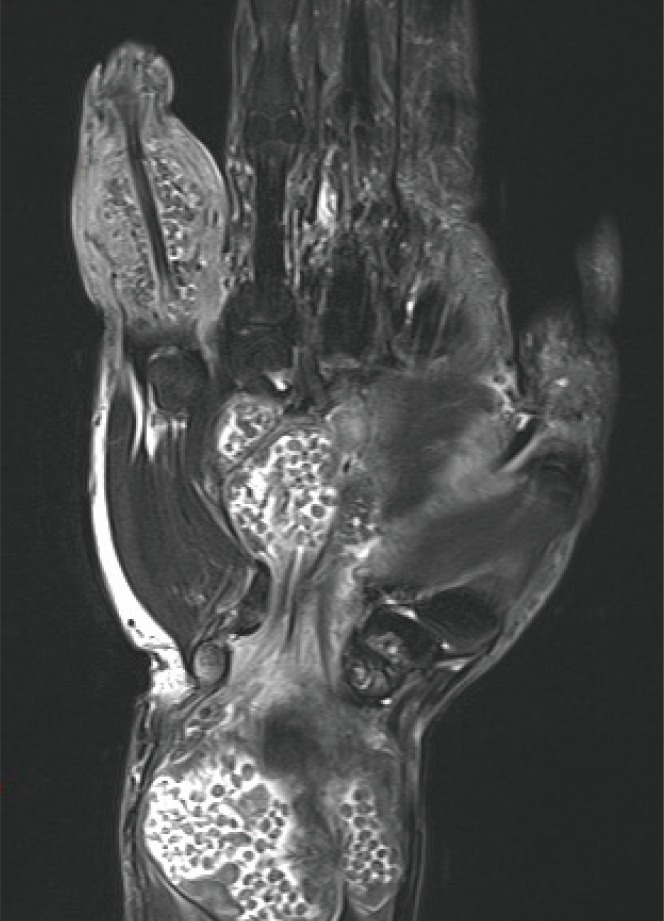
An 80-year-old male presented with enlarging masses in his left wrist, palm, and the fifth finger complaining of repetitive open wounds. The patient had no relevant medical history except a gouty attack 10 years previously. The mass first appeared in the wrist area after an acupuncture procedure following a wrist sprain 3 years previously. The mass slowly enlarged over these 3 years, and new lesions appeared on his palm and the fifth finger. His acupuncture procedure was not discontinued because of his belief that it might be helpful in removing the masses. He had fully active range of motion except in his fifth finger and no sensory change occurred. The open wound showed a wax-and-wane course during the procedure. A magnetic resonance imaging (MRI) scan revealed a wrist mass measuring 5.5 cm×5 cm×5.5 cm centered on the flexor tendon group and extensor carpi ulnaris tendon, a palm mass measuring 4.2 cm×3 cm×3.5 cm connected with the wrist mass, and a mass measuring 2.5 cm×2.5 cm×2.5 cm around the flexor digitorum profundus and the superficialis and extensor digiti minimi tendons with rice body tenosynovitis (Fig. 1). The differential diagnosis included tuberculosis tenosynovitis, rheumatoid tenosynovitis, and villonodular synovitis. An incisional biopsy through open wounds showed multiple ovoid nodules-so called rice bodies-and a histopathological examination reported chronic inflammation suspected to be a ganglion while ruling out sarcoma and giant cell tumor. A wound culture including bacteria, tuberculosis, and fungus showed an infection of Enterococcus faecalis and negative results to tuberculosis and fungus, so preoperative antibiotics were started. Complete wide excision was scheduled under regional anesthesia. Encapsulated shiny corpuscles filled with rice bodies were found surrounding the common flexor tendon sheath and extending distally to the palm through the carpal tunnel (Fig. 2). A similar mass was found on the fifth finger with a thickened flexor profundus and superficialis tendon sheath. The encapsulated masses, including the scattered rice bodies and thickened tendon sheath, were totally removed (Fig. 3). Neurovascular structures were carefully preserved. The histopathological examination showed nonspecific chronic inflammation without non-caseous necrosis. Repetitive acid-fast bacilli reactions, tuberculosis polymerase chain reaction (PCR) tests of the tissue and blood in triplicate, and additional Quanti-FERON Tb Gold (Celletis, Melbourne, Australia) in the blood all showed negative results. Evaluation for rheumatoid arthritis revealed a normal range of rheumatoid factor. Thus, we diagnosed "non-specific tenosynovitis," which did not meet the criteria for rheumatoid disease or tuberculosis tenosynovitis. The postoperative course was uneventful except for mild inflammation at the incision site (Fig. 4). It was resolved with antibiotics, and the patient showed full range of motion and normal sensory capacity after surgery. There was no recurrence at the one-year follow-up.
Rice body tenosynovitis is, rarely, reported in small case series although tuberculous tenosynovitis is relatively frequent and occurs in approximately 1% to 3% of patients with tuberculosis in endemic areas [23]. Rice bodies are non-specific findings in chronic inflammation that arise from microinfarctions with synovial shedding encapsulated by fibrin [4] and can be well observed with MRI in T1- and T2-weighted images as specific ovoid-shaped nodules of iso- or hypointense density [5].
Clinical manifestations differ depending on etiologies. In rheumatic disease, rice body tenosynovitis presents mainly in the knee joints and tendon thickness, and signal changes or ruptures frequently accompany the associated bone and joint deformities. In contrast to rheumatic disease, tuberculosis tenosynovitis does not show tendon thickness or rupture and involves small joints [4].
The histological evaluation should be performed for diagnosis in addition to clinical manifestations; multiple caseating granulomas surrounded by epithelioid histiocytes and multinucleated giant cells are typical findings, but a lack of granulomas or non-caseating granulomas is sometimes observed. Further, tissue stains for acid-fast bacilli, culture for tuberculosis, and PCR should be performed. Failure to determine the etiology, leading to a diagnosis of "non-specific" tenosynovitis, is extremely rare [3].
Since our patient had a history of multiple acupuncture treatments, we initially suspected tuberculosis or atypical mycobacterial infection based on frequent reports and clinical experiences in Asia. However, the patient's medical history, histopathological findings, PCR of the tissue and blood performed in triplicate, and repetitive cultures all excluded tuberculosis, and the etiology, in the end, remained unknown.
Complete excision including tenosynovectomy is essential even in "non-specific" rice body tenosynovitis. To prevent surgical complications, such as motor restriction or sensory changes, careful dissection should be undertaken. In the case of tuberculous tenosynovitis, more than 50% of the patients saw recurrence within 1 year. Medical therapy should therefore be used initially because of the long duration of culture growth among mycobacteria.
In conclusion, we experienced a rare case of rice body formation with unknown etiology, including large multiple mass-like lesions involving both the flexor and the extensor groups in the absence of any symptoms. Even though we should keep tuberculosis tenosynovitis in mind when rice body formation is found in endemic areas, the etiology cannot be tuberculosis and remains unknown despite repetitive diagnostic procedures. However, further studies are necessary for a better understanding of pathogenesis to establish an early treatment of disease.