INTRODUCTION
The nail apparatus consists of the nail, nail fold, nail bed (germinal and sterile matrices), and hyponychium. Fingernails usually present a longitudinal major axis, and the ratio of the width to the length (W/L) is important for the aesthetic appearance of the fingernail [1]. The fingernail is a keratinized structure with a rectangular, translucent, and transparent appearance. The fingernail covers the nail bed and is curved in both the longitudinal and transverse axes [2]. The double curvature of the fingernail enhances its resistance to mechanical stress. It has a trilamellar structure, in which the dorsal and ventral fibers run transversely, and the central fibers run in the longitudinal axis. This lamination enhances resistance to tearing and fracture forces in multiple axes [3].
A number of conditions can alter fingernail configuration. Although the fingernail W/L ratio is an important aesthetic criterion, the linear nail growth rate decreases by an average of 38% between the third and ninth decades [4]. Overcurvature of the fingernail is associated with local and systemic disorders. Transverse overcurvature of the fingernail is classified as a pincer nail, tile-shaped nail, or plicated nail. Transverse overcurvature can be observed in patients with onychomatricoma, subungual myxoid cysts, median rhomboid glossitis, and systemic sclerosis [5].
Although the shape and curvature of the fingernail can be diagnostic clues for various diseases, little is known regarding normal fingernail configuration. The aim of the present study was to characterize normal fingernail configuration and to define baseline values for comparison with abnormal conditions by measuring the fingernail W/L ratio and transverse fingernail curvature. In addition to measuring baseline values of normal fingernails in adults, we investigated factors that may influence the fingernail W/L ratio and transverse fingernail curvature.
METHODS
Data collection
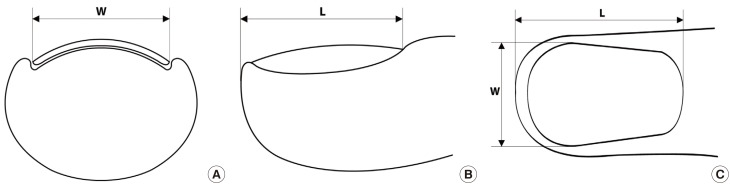
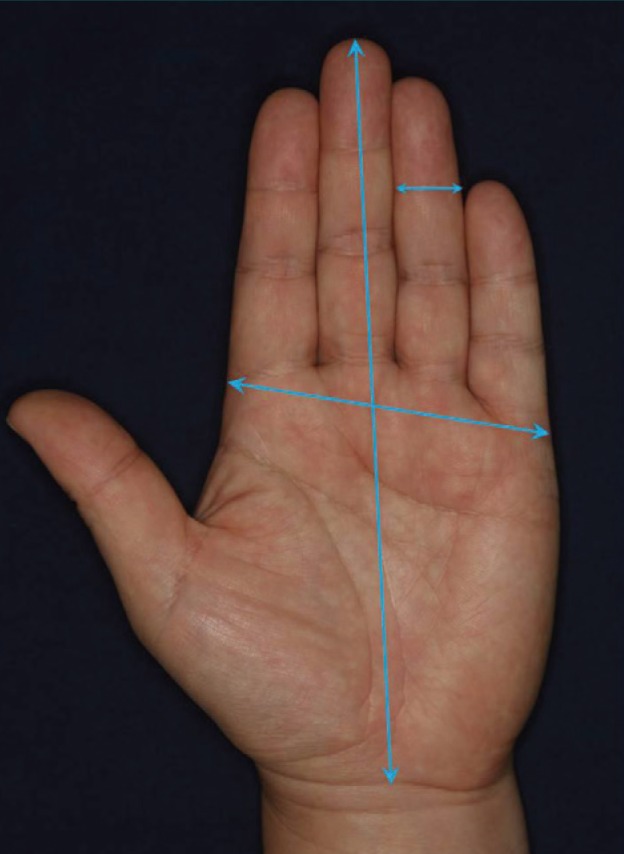
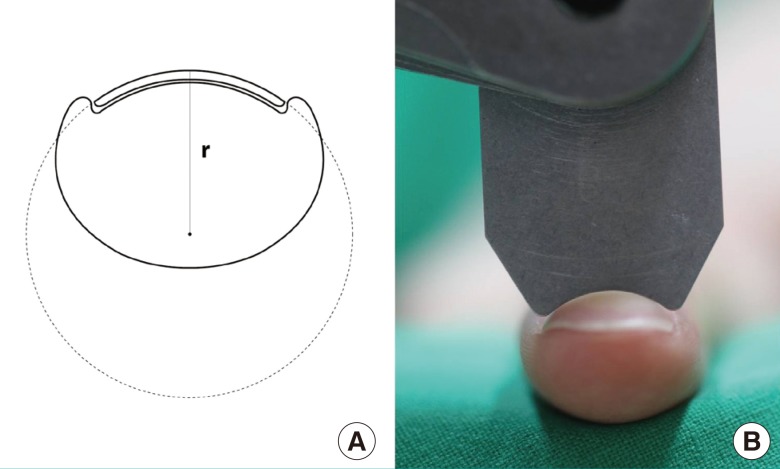
Three hundred volunteers (150 men and 150 women, with 30 subjects of each sex in their twenties, thirties, forties, fifties, and sixties) with healthy fingernails participated in this study after providing written informed consent. All study protocols were reviewed and authorized by the Institutional Review Board of Chonnam National University Hospital. Volunteers who had a history of injury or infection in their hands and/or fingernails were excluded. Participants were asked to provide details regarding age, height, and handedness. In order to evaluate the range of normal fingernail size, the W/L of each fingernail, the width of the distal interphalangeal joint (DIPJ), and the length and breadth of both hands were measured. The width of a fingernail was defined as the greatest transverse distance between the two lowest points of the fingernail in the lateral nail groove. The length of a fingernail was defined as the greatest longitudinal length between the tip of the finger and the groove at the junction of the proximal nail fold and eponychium. This definition, which used standard reference points, allowed reproducibility and prevented errors caused by variable fingernail length due to trimming the free nail margin (Fig. 1). Hand length was defined as the distance from the distal wrist crease to the midpoint of the tip of the middle finger on the palmar side. Hand breadth was defined as the distance across finger knuckles on the palmar side. The width of the DIPJ was defined as the distance across the DIPJ. Fig. 2 presents diagrams illustrating these measurements. In order to evaluate transverse fingernail curvature, we measured the radius of a circle whose curve approximated that of the fingernail plate, as shown in Fig. 3, using stainless steel radius gauges (BD178MA, 1.0-7.0 mm and BD178MB, 7.5-15.0 mm; Bluebird, Seoul, Korea). The radius gauge was placed against the surface of the uppermost part of each fingernail plate, and the radius of the curvature was recorded. All measurements were performed by one author in order to eliminate interobserver variation.
Statistical analyses
Pearson correlation analysis was used to investigate the correlation of height and hand size with fingernail configurations. The paired t-test was used to investigate the influence of handedness on the fingernail W/L ratio and the radius of the transverse fingernail curvature. One-way analysis of variance was used to investigate the influence of age on the fingernail W/L ratio and the radius of transverse fingernail curvature. Tukey's post-hoc test was used to investigate differences in the radius of transverse fingernail curvature between each age group. Differences were considered significant when P-values were <0.05. Statistical analyses were performed using SPSS ver. 18.0 software (SPSS Inc., Chicago, IL, USA).
RESULTS
General characteristics
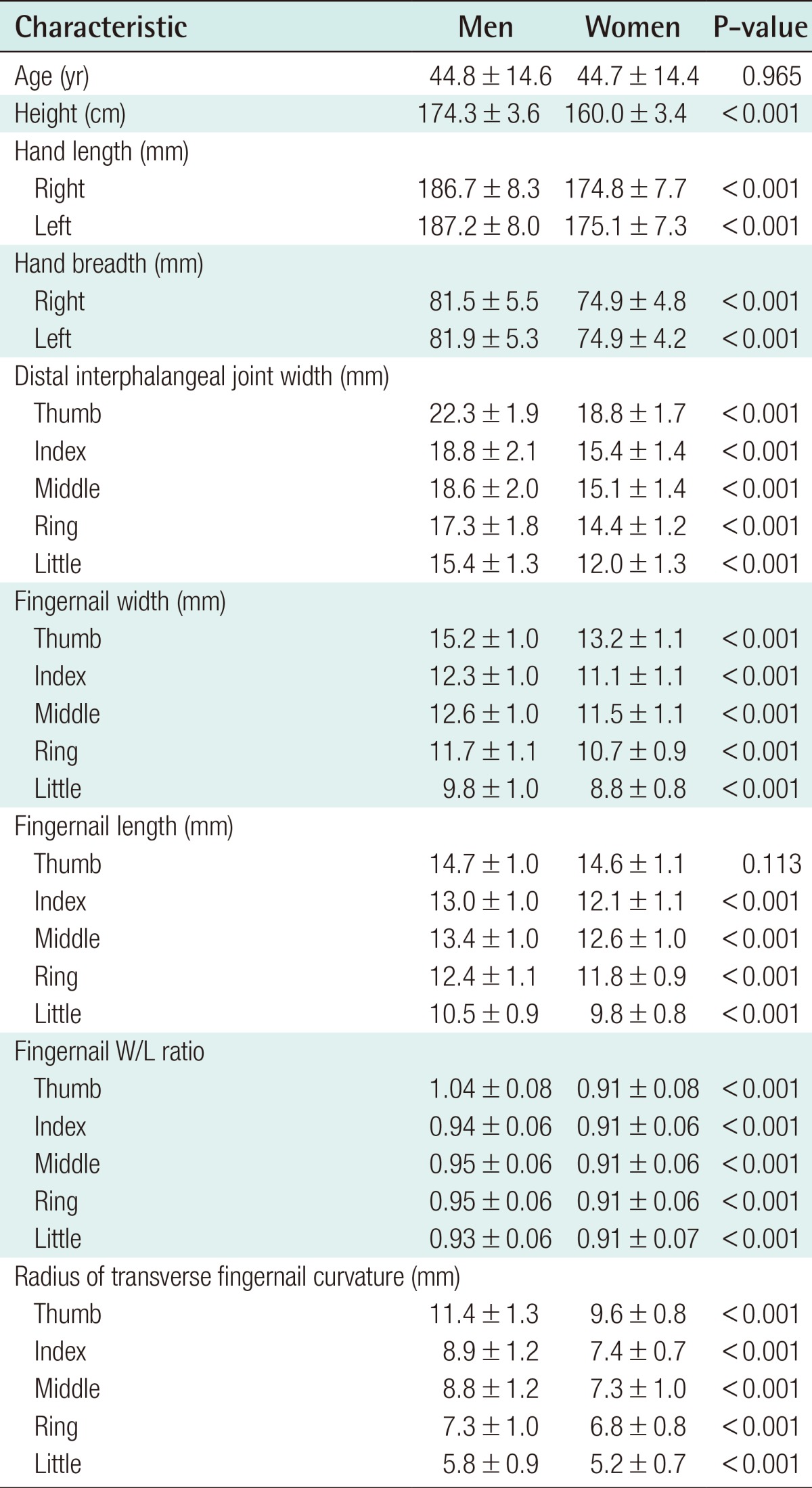
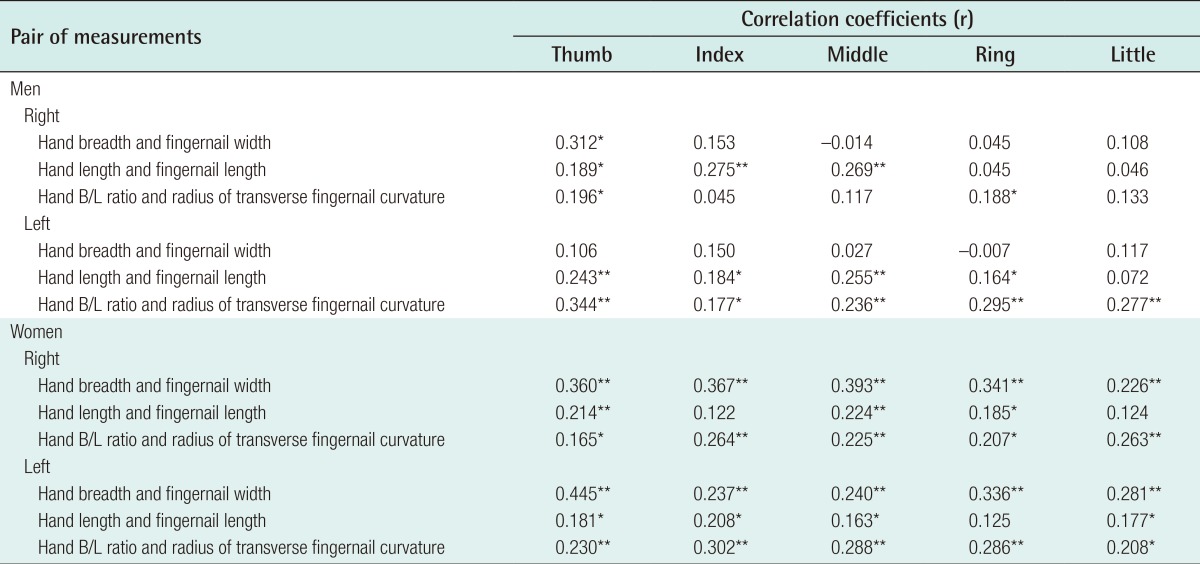
The mean age was 44.8±14.6 years in men and 44.7±14.4 years in women. Men had longer and broader hands than women. DIPJ width, fingernail width, fingernail length, fingernail W/L ratio, and the radius of transverse fingernail curvature were greater in men than in women. These parameters were also the largest in the thumb. In women, fingernail W/L ratios were similar across the five fingers, and were lower than in men. Height did not correlate with the fingernail W/L ratio or transverse fingernail curvature in any finger in either sex. The highest value of the radius of transverse fingernail curvature was found in the thumb, followed by the index, middle, ring, and little fingers. The radii of transverse curvature of the index and middle fingers were similar (Table 1). Correlations between hand size and fingernail configurations are shown in Table 2. A weak, yet statistically significant correlation was observed between the hand breadth/length ratio and the radius of the transverse fingernail curvature in all fingers in women and the left fingers only in men.
Influence of handedness on fingernail W/L ratio and radius of transverse fingernail curvature
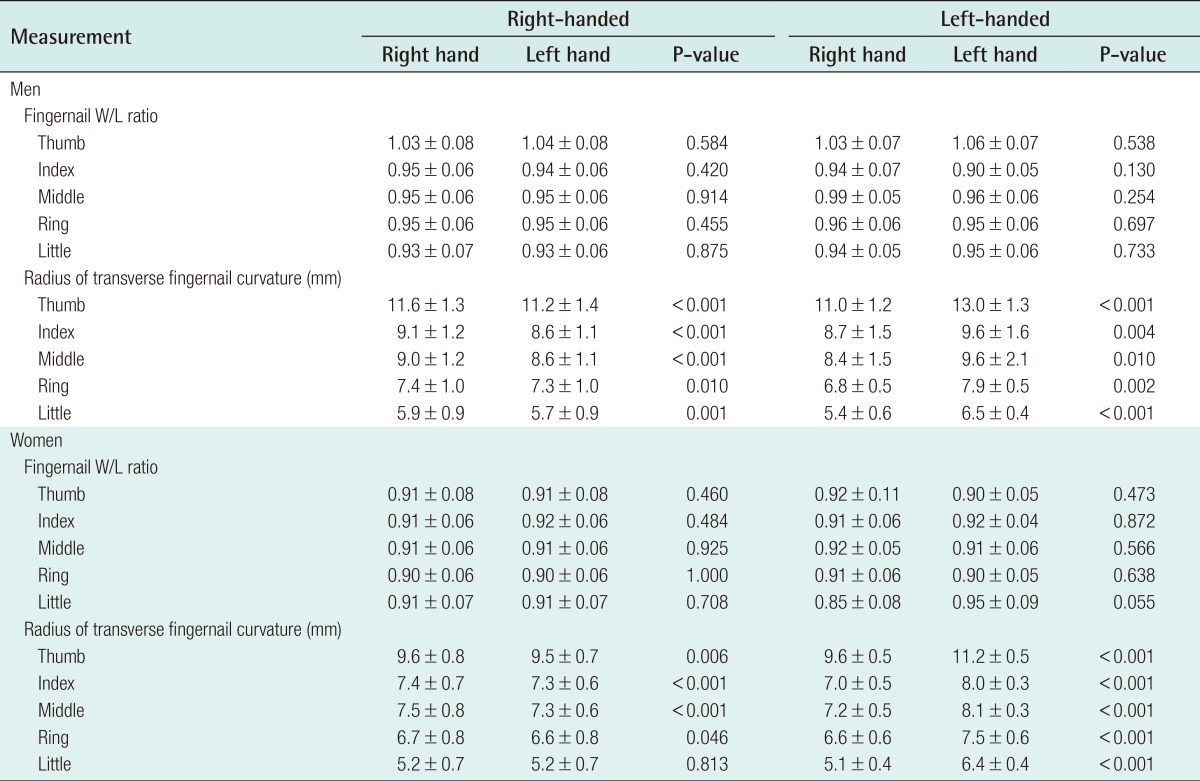
Handedness did not influence the fingernail W/L ratio. No fingernail W/L ratios demonstrated statistically significant differences depending on handedness. However, handedness did influence transverse fingernail curvature. The radius of transverse fingernail curvature was larger in the dominant hand than in the non-dominant hand. Therefore, the dominant fingernail was flatter than the non-dominant one. Statistically, the difference between the transverse fingernail curvature of the dominant and non-dominant hands was significant in all fingers in left-handed men, right-handed men, and left-handed women. In right-handed women, the difference was statistically significant in the thumb, index, middle, and ring fingers, but not in the little finger (Table 3).
Influence of age on hand and fingernail parameters
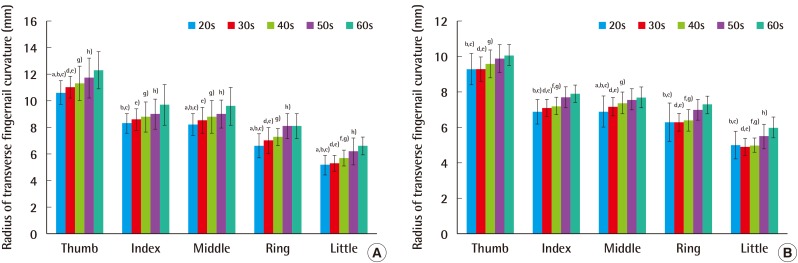
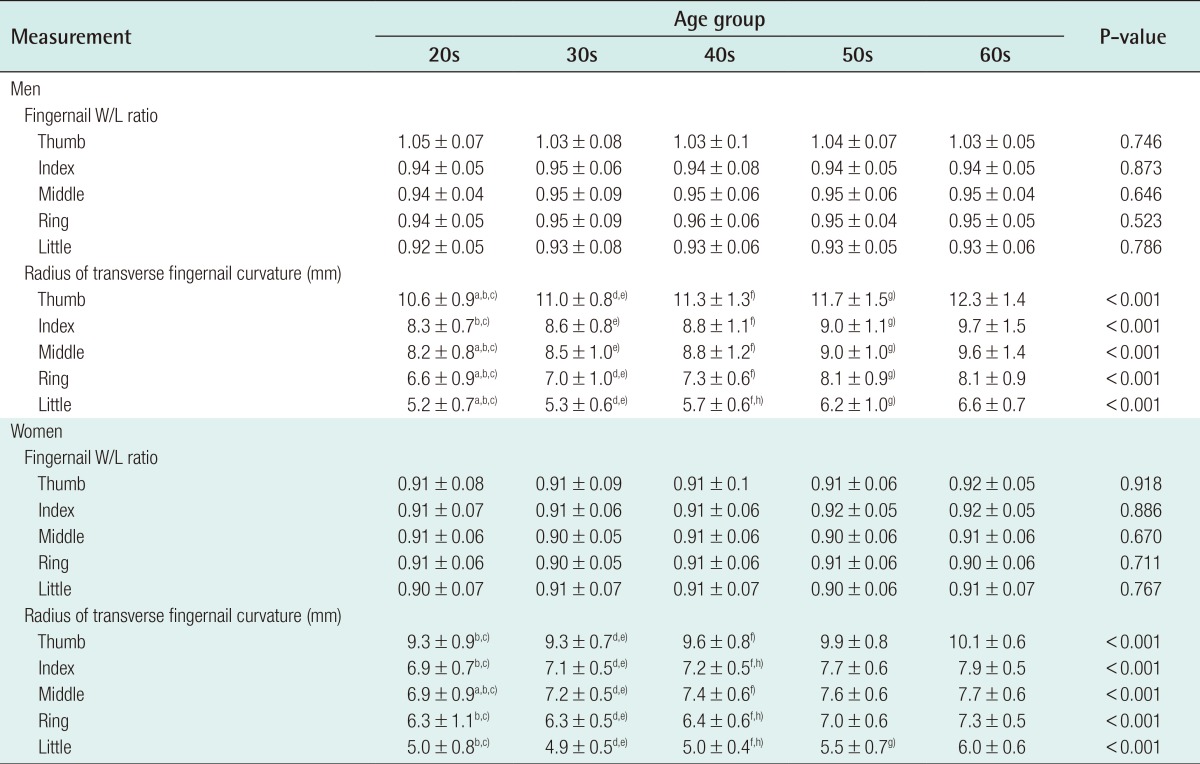
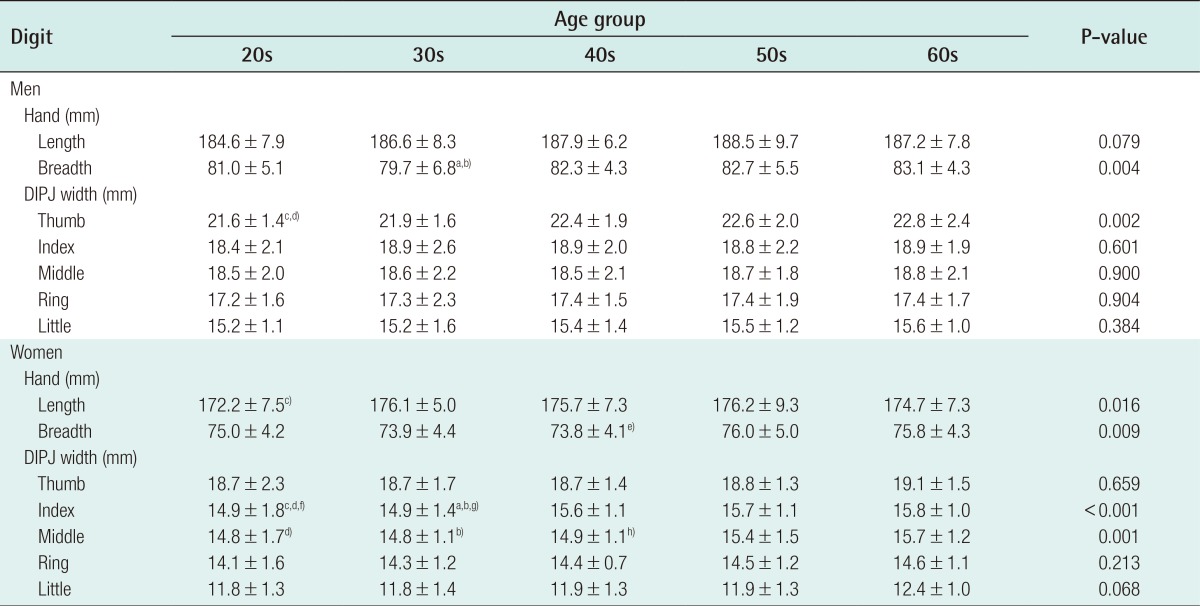
Age did not influence the fingernail W/L ratio. No fingernail W/L ratios demonstrated statistically significant differences across age groups. The radius of transverse fingernail curvature increased with age, indicating that fingernails flattened with aging. Age-related differences in the radius of the transverse fingernail curvature were statistically significant in both sexes (P<0.001) (Table 4, Fig. 4). Age-related differences in hand length, breadth, and DIPJ width are shown in Table 5.
DISCUSSION
Fingernails have numerous functions and are always exposed to physical stimulation. Fingernail configuration is influenced by genetic factors, the shape of the distal phalangeal bone, mechanical forces, malnutrition, neurogenic factors, blood flow, and factors that cause the thinning and softening of nails [6]. Widespread nail bed insults can alter the shape and size of the fingernail. Altered fingernail shapes include clubbing, pincer nails, hook nails, parrot beak nails, and koilonychia. Altered fingernail sizes include brachyonychia, dolichonychia, micronychia, and macronychia [7]. Therefore, understanding normal fingernail configuration may be important for diagnostic purposes. We measured the fingernail W/L ratio and the radius of transverse fingernail curvature. In addition to measuring baseline values of normal fingernails in adults, we investigated factors that influence the fingernail W/L ratio and transverse fingernail curvature.
The fingernail W/L ratio is important aesthetically, and some underlying diseases can alter the size of the fingernail. Brachyonychia is characterized by an increased width of the nail plate and bed relative to the length, and can be caused by nail biting, psoriatic arthropathy, hyperparathyroidism, and acroosteolysis [7]. Dolichonychia describes fingernails with excessive length compared to width and is associated with Ehlers-Danlos syndrome, Marfan syndrome, and hypopituitarism [8]. However, only a few reports have evaluated the normal fingernail W/L ratio [9]. In the present study, the mean fingernail W/L ratios from the thumb to the little finger were as follows: 1.04±0.08, 0.94±0.06, 0.95±0.06, 0.95±0.06, and 0.93±0.06, respectively, in men, and 0.91±0.08, 0.91±0.06, 0.91±0.06, 0.91±0.06, and 0.91±0.07, respectively, in women. These results reflect baseline W/L ratios of normal fingernails, and they may be useful as a reference for diagnosing brachyonychia and dolichonychia. In the present study, the fingernail W/L ratio was not found to be influenced by aging or handedness. The fingernail W/L ratio, which determines the shape of the fingernail, did not change with age. The fingernail W/L ratio also was not influenced by greater usage of a particular hand or fingers. Thus, we hypothesize that the fingernail W/L ratio can be influenced by direct injuries, including nail biting, but not by greater usage. The fingernail W/L ratio is an important factor in the diagnosis of underlying diseases and aesthetic concerns. Attractive fingernails are an important component of a well-groomed appearance, and the fingernail W/L ratio is an important feature of attractive-appearing fingernails. For aesthetic considerations, the fingernail W/L ratio should be lower than one, but fingernails that are too long are also not aesthetically appealing [10].
The fingernail covers the nail bed and is curved in both the longitudinal and transverse axes [2]. The double curvature of the fingernail enhances its resistance to mechanical stress and can be altered by systemic disorders or disorders of the fingernail itself. Under normal conditions, the upward mechanical force on the fingernail and its automatic curvature force are well balanced. However, if the upward mechanical force exceeds the automatic curvature force, the fingernail will curve outward, resulting in koilonychia. Conversely, if the automatic curvature force exceeds the upward mechanical force, the fingernail will curve inward, resulting in pincer or ingrown nails [6]. Nail clubbing, which is overcurvature in both the longitudinal and transverse axes, can be associated with pulmonary and cardiovascular diseases [7]. Pincer nail, which is characterized by transverse overcurvature of the fingernail, can be caused by subungual exostosis, osteoarthritis, onychomycosis, and ectodermal dysplasia [11]. Koilonychia or spoon nail, which presents as a concave fingernail, can be associated with anemia, thyrotoxicosis, acromegaly, nail psoriasis, onychomycosis, and lichen planus. In this study, the respective radii of transverse fingernail curvature from the thumb to the little finger were 11.4±1.3 mm, 8.9±1.2 mm, 8.8±1.2 mm, 7.3±1.0 mm, and 5.8±0.9 mm, respectively, in men, and 9.6±0.8 mm, 7.4±0.7 mm, 7.3±1.0 mm, 6.8±0.8 mm, and 5.2±0.7 mm, respectively, in women. The ordering of the radius of transverse fingernail curvature reflected the size of the fingers at the distal phalanx, and men had flatter nails than women. In comparison with a previous study conducted in England [12], we observed a smaller radius of transverse fingernail curvature in all fingers. This finding seems to reflect smaller measurements of DIPJ width and hand breadth. Our results provide baseline values for normal transverse fingernail curvature in diagnosing overcurvature of the fingernail in Koreans.
Handedness was found to influence transverse fingernail curvature. The radius of transverse fingernail curvature was significantly larger in the dominant hand than in the non-dominant hand. Therefore, the dominant fingernail was flatter than the non-dominant one. The influence of hand dominance on transverse fingernail curvature suggests that the greater usage of particular hands and fingers leads to flatter fingernails [12]. Age also influenced transverse fingernail curvature. The radius of transverse fingernail curvature significantly increased with age, indicating that the fingernails flattened with aging. DIPJ width increased with age in some fingers (the thumb in men, and the index and middle fingers in women). It appears that the increase in the transverse fingernail curvature radius with age is not the result of increasing DIPJ width. Various changes to the fingernail can be caused by aging and affect transverse fingernail curvature. With increased age, the linear nail growth rate is decreased, and the contour is modified, resulting in platonychia and koilonychia [13]. The longitudinal ridges become more pronounced and numerous, and the color varies from shades of yellow to grey. The chemical composition of the fingernail changes with age, showing a decreased calcium concentration [14]. Our finding that handedness and aging are associated with transverse fingernail curvature suggests that fingernails become flatter with age and greater usage.
The primary limitation of our study is that it was conducted on a small population drawn from a single city in Korea. Therefore, further large-scale studies investigating fingernail configuration according to age or race may help to generalize our normative data. In addition, further studies that investigate the fingernail configuration of patients who have diseases that may alter the fingernail shape are needed.
In this study, we measured the fingernail W/L ratio and transverse fingernail curvature, and reported baseline values of normal fingernail configuration in adults. These normative data on fingernail configuration may be valuable for use as a reference range in the diagnosis of various diseases and deformities of the fingernail and for patients undergoing reconstructive or aesthetic fingernail surgery.