INTRODUCTION
Healthcare innovation has shaped the evolution of plastic surgery in the last century. Perhaps the most historic demonstration of such was the pioneering work of Sirs Harold Gillies and Archibald McIndoe in the World Wars of 1914 and 1939 [12]. Since then, both invention and implementation of new technologies have continued to facilitate advances in patient outcomes and opportunities in plastic surgery.
Outside of the healthcare literature, the study of the process of innovation (i.e., diffusion of innovation) is a mature field originating from the observations of social scientists in the mid-twentieth century [34]. Patents and publications are well-documented measures of innovation and exist in vast numbers detailing technological advances in surgery. Although articles exist in the healthcare literature relating to the diffusion of innovation, many focus on healthcare processes with few offering an objective or quantitative view of the diffusion of technological innovation [5].
Key plastic surgical innovations, in the context of both research and clinical medicine, listed in the literature include microsurgery, breast surgery, liposuction, tissue engineering, transplantation, and laser technology [67]. These suggestions were made on the basis of significant professional experience, but a distinct lack of evidence. Recent work has demonstrated the utility of publically available patent and publication data to quantify innovation within surgery and proposes a novel methodology for assessing areas of technological innovation [8910].
Such systematic approaches to horizon scanning for new evidence of innovation poses significant opportunities and implications within research-funding bodies and investors alike. Current strategies for directing the nature of calls for proposals, as well as choosing those that are supported, might be more reliably guided by more robust technology trend analyses. Furthermore, reviewing these historical data might better inform academic programmes when appraising and advancing research angles.
The objectives of this paper are: first, to identify and characterise the most prevalent areas of innovation in plastic surgery using patent and publication data; and second, to evaluate key areas of innovation outlined by experts in the literature.
METHODS
Patent and publication data retrieval
Patents from over 90 countries and publications for plastic surgery between 1960 and 2010 were retrieved using the proprietary software PatentInspiration (Aulive, Ypres, Belgium) and PubMed (National Library of Medicine, Bethesda, MD, USA). The Boolean search strategy ("plastic surgery" OR "plastic surgeon" OR "plastic surgical") was used, limiting the results to single members of patent families in order to prevent duplication. Data for patent and publication activity were normalised using an innovation index as described by Hughes-Hallett et al. [8]. The innovation index is calculated by dividing the number of publications or patents in a given year by the total patent and publication counts from 2010 ('present day'). This has the effect of highlighting change in activity beyond that caused by natural growth in industry and the population.
Top performing patent codes
Every patent filed is classified using one or more standardised hierarchical codes, e.g., 'A61F2/12' for Mammary prostheses and implants. The 50 most prevalent patent codes associated with the technologies retrieved from the database search were identified and grouped under subheadings chosen by the authors. Assignment of codes into technology areas was conducted independently by 2 authors (R.M.K. and H.J.M.), with any disagreement being resolved by a third (A.H.H.). Patents related to pharmaceutical products were omitted. This process was repeated each decade to explore change over time.
The activity of the top performing technology areas was investigated further through specific searches of patents and publications. Search terms were built and modified to minimise the appearance of unwanted results on a case-by-case basis. For example, in cases where search terms might be considered generic, such as 'device', patent searches were limited to results in which the term was present in the title or abstract. Normalised data were plotted graphically to facilitate the assessment of growth patterns. To account for smaller datasets related to specific technologies, moving averages were employed in order to ease interpretation.
Statistical analysis
Evidence suggests that a high correlation between patents and publications during periods of growth is indicative of substantial innovation [11]; therefore, correlation coefficients were calculated. In the case of a monotonic relationship, Pearson's or Spearman's rank was used for linear or non-linear associations, respectively. The coefficient of determination (R2) was used to quantify and compare the fit of data to linear and exponential trend lines. Statistical analysis was performed using the IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA).
RESULTS
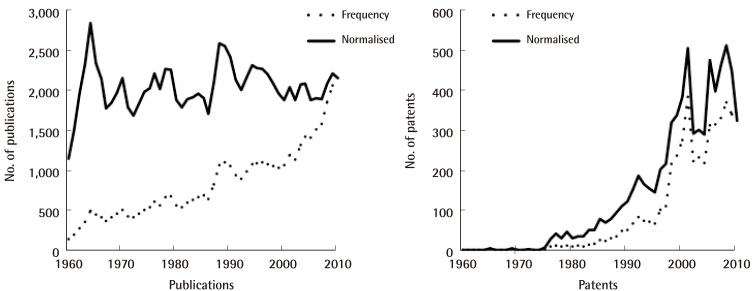
In plastic surgery between 1960 and 2010, 4,651 patents and 43,118 publications were retrieved. After normalisation, the publication activity appeared to be steady, whereas patent activity exhibited an exponential rise (R2 exponential=0.85) (Fig. 1).
Between 1960 and 2010, the top performing technology groups were reconstructive prostheses, non-invasive practices, surgical instruments, implants, and tissue engineering (Table 1).
Technologies related to surgical instruments were the most active in terms of patent filing in the 1980's. In the last two decades, patents related to reconstructive prostheses have become the most prevalent, with instruments and non-invasive techniques comprising the majority of the remaining technologies (Table 2). Patents related to pharmaceutical products were omitted (1980's, 8; 1990's, 16; 2000's, 17; 1960–2010, 19).
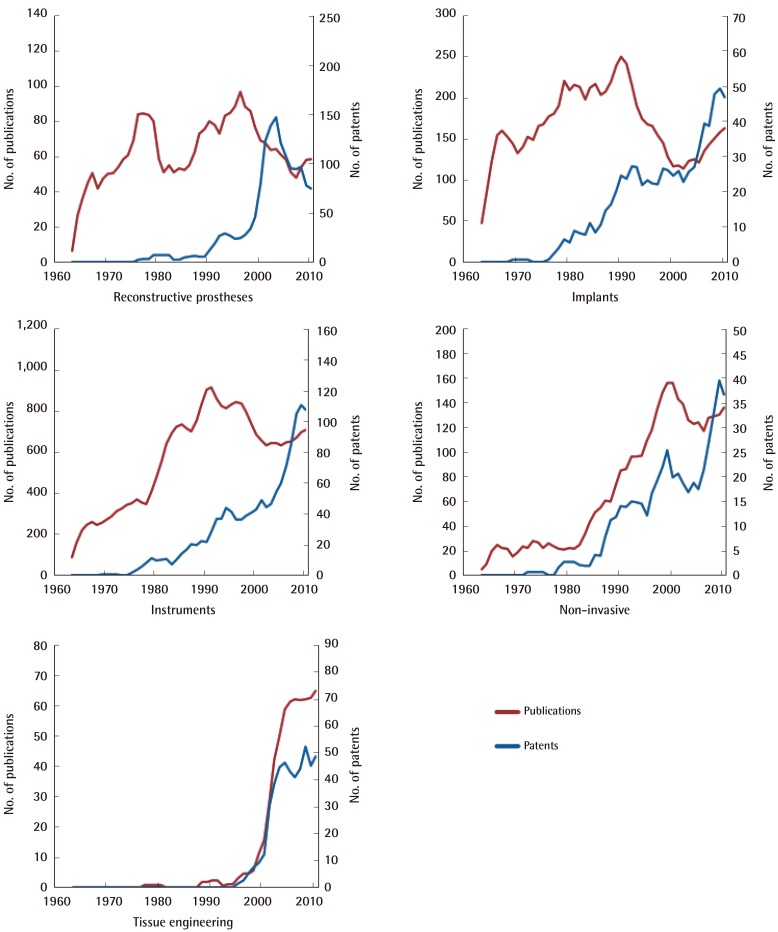
Of the top performing technology areas (Table 3), instruments, non-invasive technologies and tissue engineering all have strong correlations between patent and publication activity (range Spearman's rank, 0.678–0.893; P<0.001). Implants, instruments and non-invasive technologies all appear to be undergoing growth, whilst reconstructive prostheses and tissue engineering have shown convincing plateaus. Of the growing technologies, instruments and non-invasive technologies both show greater concordance with exponential lines of best fit (average exponential vs. linear R2=0.8 vs. 0.7), whilst implants rise in a more linear fashion (R2=0.6 vs. 0.7) (Fig. 2).
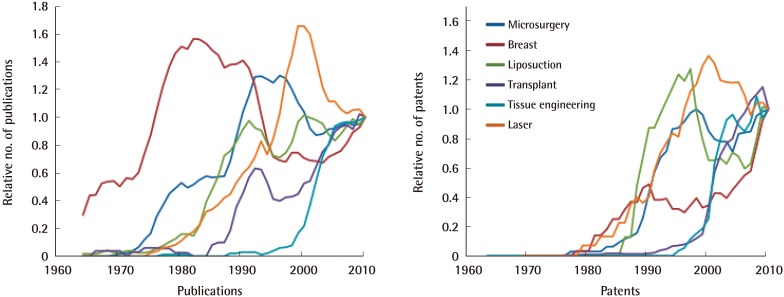
Microsurgery (within plastic surgery) accounted for 156 patents, following a sigmoidal growth curve plateauing in 2000. Breast surgery (109 patents) appeared to exhibit potentially two distinct growth phases—first in the 1980's and again in the late 2000's. Liposuction (34) underwent rapid growth almost immediately on conception in the late 1980's, which was unsustainable. Tissue engineering (403) and laser technologies (104) both exhibited sigmoidal growth curves with plateaus in the mid- and early 2000's, respectively. Patents related to transplantation (649) display a dramatic exponential growth phase around the year 2000, which is only very recently showing signs of cessation. Of the growing technologies, transplantation was strongly exponential (exponential vs. linear R2=0.7 vs. 0.3), whereas breast surgery was mostly exponential (R2=0.5 vs. 0.4) in its growth trend. The correlations between patents and publications were all statistically significant, with all apart from breast being strong (R>0.7) (Fig. 3).
DISCUSSION
A novel innovation metric was applied to the field of plastic surgery showing exponential growth in patents over the last 50 years, with a relatively fixed related publication output. This is an expected finding, considering that healthcare patents are outperforming patents in general (the latter of which were used for normalisation). The top performing patent codes, and therefore areas of innovation, were identified as reconstructive prostheses, tissue engineering, implants, instruments, and non-invasive techniques, of which the latter 3 are currently in growth. Expert-derived innovation areas were also evaluated, highlighting the differences (and similarities) between different technologies with respect to time of conception, growth patterns, and the current state of flux.
The Diffusion of Innovation theory described by Rogers proposes that the technology adoption curve is sigmoidal, with a period of incubation prior to widespread adoption, followed by technological refinement [3]. The data displayed in this work facilitates guided speculation with regard to forecasting future areas of growth by establishing the current phase of innovation in a particular technology. Technologies currently experiencing growth include surgical instruments, implants, non-invasive techniques, transplantation, and breast surgery. Of these technologies, transplantation is visually and statistically the most exponential, with a concurrent boom in associated publication activity. This is in keeping with the current interest in vascularised composite allotransplantation, both from expanding case series (including the first hand transplant in the UK in 2013) [1213] and novel strategies for inducing immune tolerance [1415] that address the ethical constraints associated with long-term immunosuppression [16].
The correlation between publications and patents of the majority of the technology groups were strong, suggesting substantial innovation. However, patents and publications for reconstructive prostheses and implants were poorly correlated. Publication activity in these areas emerges rapidly in the 1960's before plateauing, whereas patents activity rises later on with little impact on publication activity. A poor correlation between publications and patents has previously been explained by periods of technology refinement, where mature technologies are incrementally refined by industry to maintain market share, rather than to modify clinical practice [11].
The majority of innovations listed by senior plastic surgeons were reassuringly represented in the top performing patent codes. Overarching technology areas are likely to envelop niche patents, such as liposuction and negative pressure dressings falling under instruments, for example. Simple and useful technologies such as liposuction exhibit rapid uptake with a befitting exponential rise, before falling away as the limited number of plausible amendments or advances are exhausted.
Microsurgery is undoubtedly one of the most disruptive innovations in plastic surgery [17]. After Jacobson and Suarez achieved the first experimental microvascular anastomosis using an operating microscope in 1960 [18], a prolonged incubation phase saw various microsurgical cases documented, such as the first arm replant in 1964 [19]. It was only after the assembly of the International Society of Reconstructive Microsurgery in 1972 that the technique began to be more widely adopted, with a subsequent surge in patent activity.
The patent activity of half the technologies explored has plateaued. It is possible that other emerging innovations in plastic surgery have been missed. It is also likely that innovation is occurring in other surgical specialties, to be adopted by plastic surgeons in due course. Hughes-Hallett listed the key areas of innovation in surgery as minimally invasive surgery, robotic surgery, surgical staplers, and image guidance, with robotics and image guidance very much in the exponential phase of growth [8]. Use of robotic platforms for microvascular anastomosis or neurorrhaphy [20], imaging for locating perforating blood vessels [21], and planning surgical reconstruction [22] are beginning to be described in the plastic surgical literature.
Amongst other interesting findings, patient record management was the top performing plastic surgery patent in the 2000's (aside from skin preparations). Similarly, this decade sees the emergence of the patent code for software for market research and analysis. This suggests that the focus of innovation is expanding to address more holistic aspects of the healthcare process, including managing and extracting information from so-called 'big data' to optimise care pathways whilst maintaining a robust healthcare business model.
Although the methodology used provides new insight into innovation in plastic surgery, it is not without limitations. As with systematic reviews, building search terms is an inherent source of bias. To minimise bias, search terms were kept concise, avoiding listing specific technologies to add to or limit the search where possible. Also, the same search terms were used for patents and publications, regardless of differences in article architecture. Additionally, the results generated from nonspecific patent search terms such as 'device' were restricted to those found in the title or abstract and not the description, which can often include a broader discussion of technology components not central to the innovation in focus in the patent.
Reconstructive prostheses comprise a large industry, which spans multiple specialties. Whilst such technology may be more typically associated with orthopaedics, the wide applicability and the format of the patent applications result in it being a major feature in this study. Plastic surgery is unique in that the specialty is not confined to a single organ or organ system, which makes defining a search strategy more challenging. The study methodology was more likely to be overly inclusive rather than incomplete, as any technology that may be encountered by a plastic surgeon is likely to be listed in the patent application.
Furthermore, patent records are such that any patent may fall under more than 1 code, potentially leading to over-representation of a particular patent when assessing the top performing patent areas. It is conceivable that this phenomenon is skewed towards certain technology areas, for example a new multi-modular hip prosthesis with a smart coating may result in 5 or more 'hits' on various prosthesis-related patent codes (Table 1), whereas a breast implant has fewer possibilities. Conducting patent searches using expert-derived technologies in addition to those representing top performing patent codes ensures areas of interest are not disregarded.
The application of a novel metric for evaluating innovation in plastic surgery generated a natural history of technologies fundamental to the evolution of the specialty. This methodology has revealed which technologies are currently undergoing growth, providing unique insight into the expected landscape of clinical and academic plastic surgery in the decades to come. Future work may look to advance the methodology in order to detect the features of emerging technology groups that may be able to predict uptake and ultimately success. Learning from historical trends in patents and publications, along with additional supplementary metrics, might allow the most promising 'seedlings' to be selected and nurtured through direct resource allocation. This method has the potential to fast track the development and translation of new disruptive technologies into the healthcare domain.