INTRODUCTION
When skin cancer is clinically suspected, biopsy is usually performed preoperatively for histopathological diagnostic confirmation. Then, according to the results of the biopsy, it is decided whether further surgery is necessary. When a skin lesion is highly suspected of malignancy upon physical examination by a surgeon or a dermatologist, full excision followed by a frozen biopsy is sometimes performed. If the results of the frozen biopsy show malignancy, a further wide excision is performed directly for complete excision.
In the case of malignant melanoma, studies have been performed for decades to determine whether cutting into a malignant melanoma, a so-called preoperative biopsy, leads to a worse prognosis for the patient, but it is still an object of controversy [1]. However, there are no reports about the effects of preoperative biopsy on recurrence of basal cell carcinoma (BCC) or squamous cell carcinoma (SCC). The aim of this study is to evaluate whether preoperative biopsies of BCC or SCC had affected recurrence after operation.
METHODS
Patients and methods
Primary BCC or SCC patients who underwent standard surgical excision with hospitalization between 1991 and 2010 were retrospectively reviewed. We collected information including age, sex, tumor location, size in maximal dimension, and time interval from preoperative biopsy to first operation. Preoperative biopsies included excisional biopsy, incisional biopsy, and punch biopsy.
Among the 102 BCC patients and 127 SCC patients, the patients who met the exclusion criteria were excluded, and 45 BCC patients and 54 SCC patients were ultimately analyzed. The exclusion criteria included recurrent cases, absence of distinct information about biopsy, follow-up duration of less than one month, and post-operative follow-up loss.
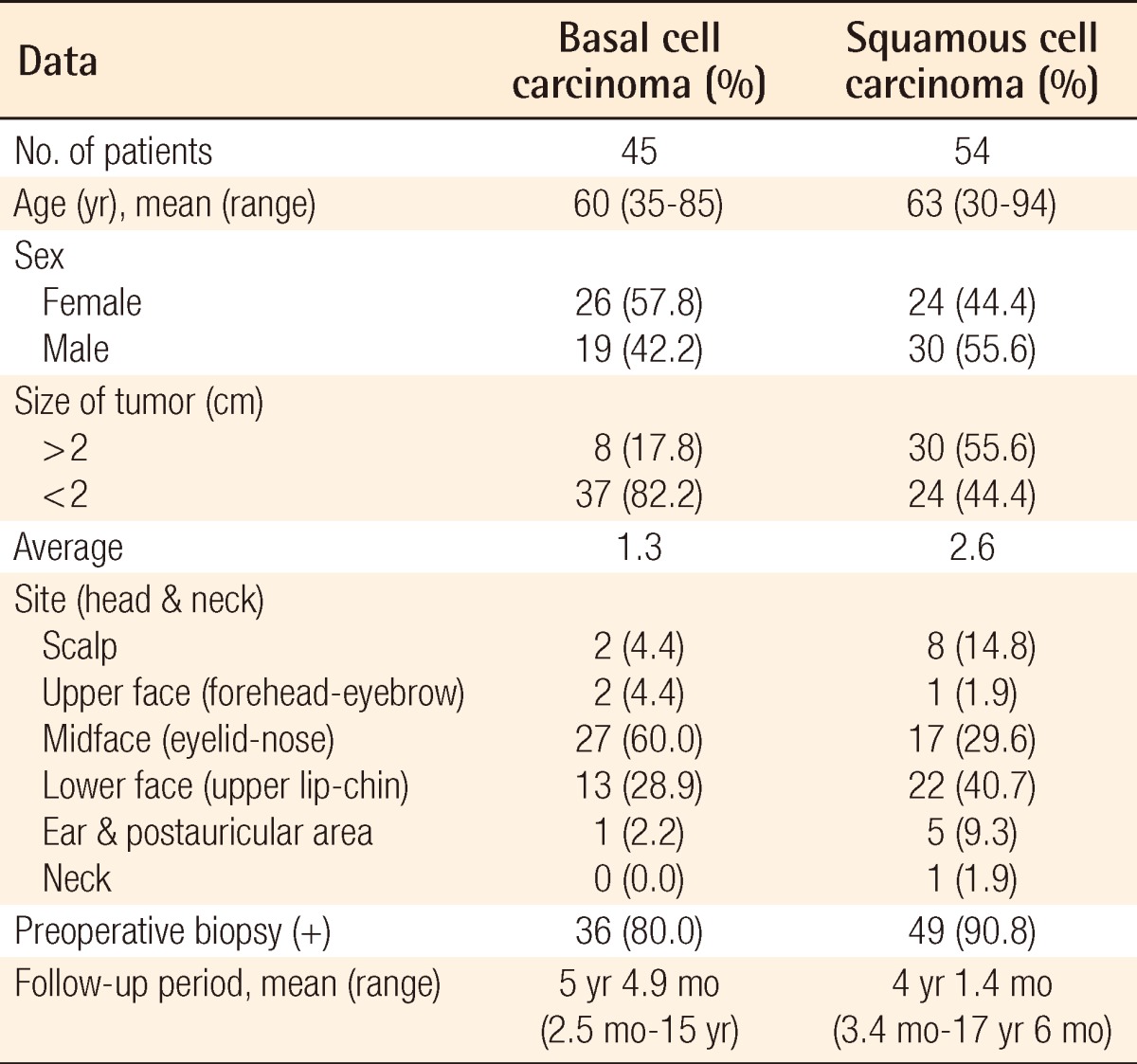
The mean age of the BCC patients was 60 years old (range, 35 to 85 years old) and that of the SCC patients was 63 years old (range, 30 to 94 years old). The female-to-male ratio was about 1.37:1 among the cases of BCC and 0.8:1 among the cases of SCC. The average tumor size in maximal dimension was 1.3 cm in the BCC patients (range, 0.1 to 8.5 cm) and 2.6 cm in the SCC patients (range, 0.2 to 14.5 cm). The most common site of BCC was the midface, especially the nose, and that of SCC was the lower face, especially the cheek. The preoperative biopsy rate was 80.0% among the BCC patients and 90.8% among the SCC patients. The definition of "follow-up period" is from the operation day to the last visit. The mean follow-up period was 5 years and 5 months in the BCC patients (range, 2.5 months to 15 years) and 4 years 1 month in the SCC patients (range, 3 months to 11 years 8 months) (Table 1).
To prove the effect of preoperative biopsy on recurrence of BCC and SCC, the recurrence rates of BCC or SCC with and without biopsy were compared, respectively, using a logistic regression analysis, controlling for confounding factors including age, sex, and tumor size [2]. Furthermore, to confirm the relationship between the interval from biopsy to operation and postoperative recurrence, a logistic regression analysis was performed among the biopsy groups. The data were analyzed using the SAS ver. 9.1.3 (SAS Institute Inc., Cary, NC, USA) statistics program.
RESULTS
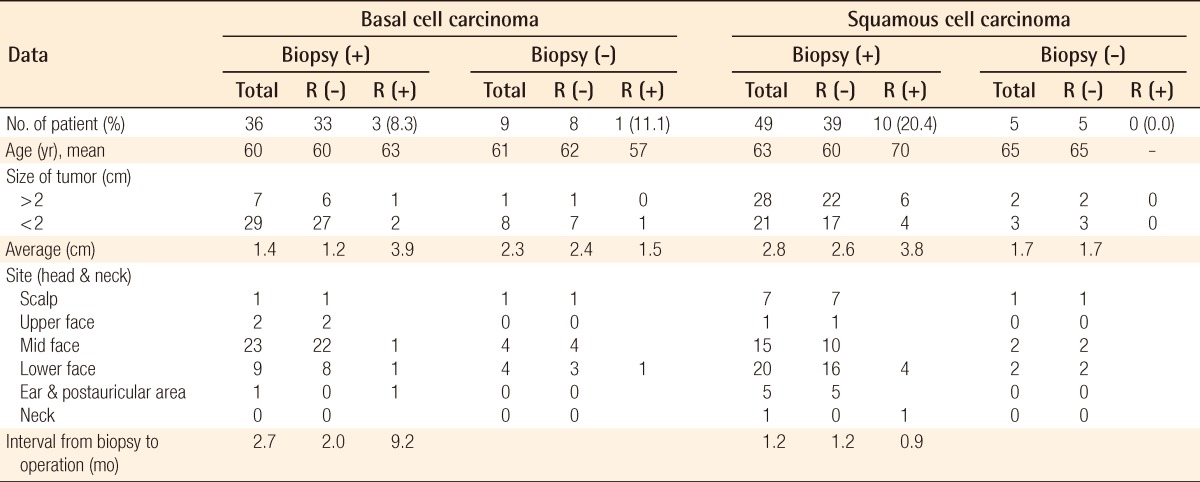
The composition of the groups is summarized in Table 2, which were divided according to whether or not diagnostic biopsy was performed preoperatively. There was no significant difference in terms of confounding factors including age, sex, or tumor size between the two groups. Each group was subdivided by tumor size above (high risk) and below 2 cm (low risk), and statistical analysis was performed. There was no statistically significant difference in the proportion of high risk cases between the two groups, which means that the compositions of each group in terms of severity had little difference.
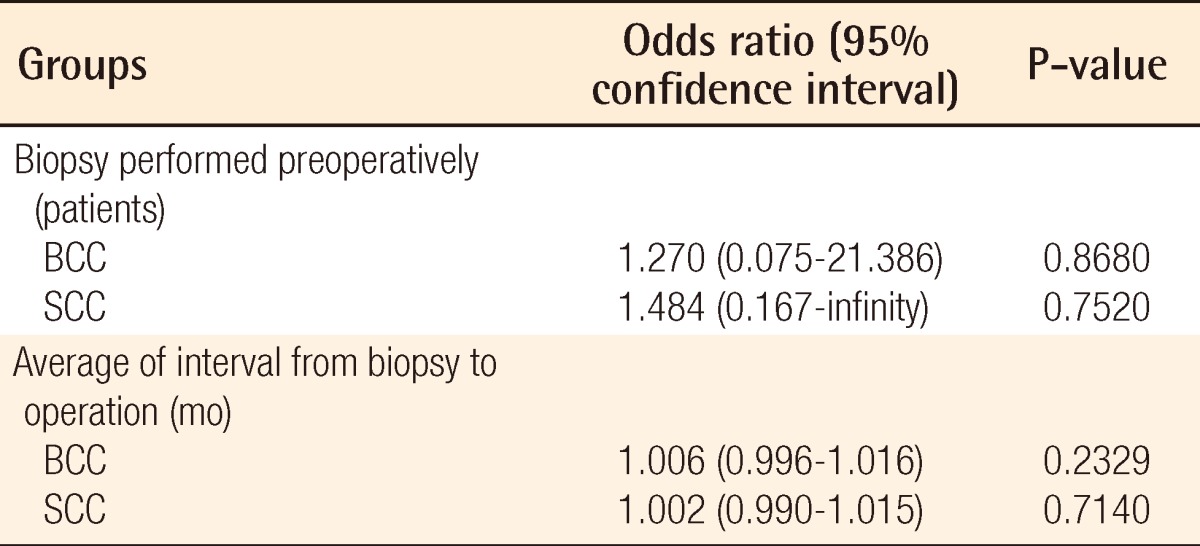
Among the cases of BCC, the recurrence rates with and without biopsy were 8.3% (n=3) and 11.1% (n=1), respectively. The recurrence rates of SCC with and without biopsy were 20.4% (n=10) and 0.0% (n=0), respectively. For cases with biopsy performed compared to non-biopsy cases, the odds ratio of recurrence was evaluated. There was no statistically significant association between preoperative biopsy and recurrence (Table 3). The mean interval from biopsy to operation was 9.2 months (range, 20 days to 2years) among the BCC patients who had recurrence, whereas that of those who had no recurrence was just 2.0 months (range, 6 days to 6 years), which was much shorter than the recurrence group. In the group with SCC who underwent biopsy, the mean interval from biopsy to operation was 0.9 months (range, 14 days to 5 years) among the SCC patients who had recurrence, whereas that of those who had no recurrence was 1.2 months (range, 11 days to 10 months). The interval from biopsy to operation had no statistically significant association with recurrence (BCC, P=0.2329; SCC, P=0.7140) (Table 3). Among the BCC group members, the average tumor size was 1.2 cm in the patients without recurrence and 3.3 cm in the recurrence patients. Among the SCC group members, the average tumor size was 2.5 cm in the patients without recurrence and 3.8 cm in the recurrence patients. To clarify whether tumor size independently affected the recurrence of BCC or SCC, we performed a statistical analysis using a t-test, but there was no significant relationship between size and recurrence (BCC, P=0.3516; SCC, P=0.3435).
DISCUSSION
Skin cancer is the most common malignant tumor in humans. BCC and SCC are the two most common types of skin cancers. Exposure to ultraviolet radiation is generally accepted as the major cause of skin cancer, so it occurs most frequently in the head and neck region that is exposed directly to the sun [3].
Basal cell carcinoma is usually a slow-growing and locally invasive tumor that rarely metastasizes, although its characteristics depend on histological variants. The risk factors associated with extensive subclinical spread include a tumor diameter greater than 2 cm, location on the central part of the face or ears, long-standing duration, incomplete excision, an aggressive histological pattern of growth, and perineural or perivascular involvement [3,4].
Squamous-cell carcinoma in situ may progress to invasive disease if it is not completely removed [5]. Most invasive squamous cell carcinomas occur on the head and neck area. The representative risk factors for recurrence and metastasis of squamous cell carcinoma are size and location of the tumor, specifically the lip, ear, and scalp area [6].
There are two main reasons why incisional biopsy is performed preoperatively rather than by directly excising the tumor. First, curative surgery of skin cancer requires a wider excision margin, so it can be aesthetically hazardous. Second, in cases with low suspicion of malignancy, it is unnecessary to directly excise the tumor [7]. Therefore, preoperative biopsy of a skin tumor of the head and neck has become generally accepted. Following this practice, the majority of patients at our institute underwent preoperative biopsies (BCC, 80.0%; SCC, 90.7%).
However, some reports of the negative effects of mechanical manipulation have been published [8,9]. Whatever the type of biopsy, cutting the tumor itself entails the possibility of seeding malignant cells and can induce metastasis. Austin et al. reported that cutting into a cutaneous melanoma could seed cells directly into the bloodstream, leading to a higher risk for distant metastases and worse overall survival in the biopsy group [8]. Many studies have been performed over the past few decades to determine whether cutting into a malignant melanoma leads to a worse prognosis for the patient, but this is still an object of controversy [1]. In this study, preoperative biopsy did not show any statistical significance for the recurrence of BCC or SCC.
BCC metastasis via the lymphatics or blood is known to be extremely rare. The recurrence rate of BCC after definite surgical excision is known to range from 0.0028% to 0.55% [3]. In this study, the recurrence rates of BCC with and without biopsy were 8.3% and 11.1%, respectively, which are much higher than the established values. Many of the patients were referred to our hospital after being diagnosed by biopsy at other institutes or clinics, and our hospital is a tertiary center belonging to a medical institute. Thus, there might be a higher incidence of severe cases than at average hospitals. In the cases of BCC, the average interval from biopsy to operation in the recurrence group was 9.2 months, which was much longer than that in the group with no recurrence (2.0 months). Even though there was no statistical significance, this shows the tendency towards recurrence of BCC with longer delays. If more patient data were collected, this could be clarified. However, this tendency suggests that definite surgical excision should be performed as soon as possible after biopsy.
Regarding the SCC, the recurrence rate of the biopsy group was 20.4%; however, there was no recurrence among the patients who had direct definite surgery. In other words, there was no recurrence in those with SCC who did not have preoperative biopsy. Even though the number of patients without biopsy was only 5, this result can suggest some possibility of a negative effect of biopsy in SCC. However, there was no statistical significance; because the number of patients in the SCC group without biopsy was "zero," there were limitations to the reliability of the statistical analysis. Certainly, more patient data should be acquired and analyzed for statistical confirmation. The chief risk factors for SCC recurrence are known to be the size (>2 cm in diameter) and location of the tumor. However, in our results, there was no statistically significant relationship between size and recurrence, which means there could be complex factors besides tumor size that affect recurrence.
There are several concerns that limit our ability to generalize these results. The main limitation is the small number of patients who did not undergo a preoperative biopsy because we only included patients who had reliable medical records. In light of these results, authors recommend the definite surgery of skin cancer as soon as possible after clinical or pathological diagnosis.
Preoperative biopsy of skin cancer did not show a statistically significant influence on recurrence of BCC or SCC. However, in the cases of BCC, there was a tendency toward recurrence among those with a longer interval from biopsy to operation. This result supports definite treatment as early as possible after the preoperative biopsy for patients' safety. There were no hazardous relation between preoperative biopsy and recurrence of SCC and BCC, statistically. However, once the diagnosis is confirmed clinically or pathologically, definite surgery is recommended as soon as possible.