INTRODUCTION
Fingertips are highly susceptible to trauma, but they are also an essential part of the hand for both functional and esthetic reasons. Since the first successful finger replantation by Komatsu and Tamai [1], there has been much progress in microsurgical fingertip replantation and reconstruction distal to the distal interphalangeal joint [2]. However, in distal digital microsurgery, the main technical difficulty is venous repair [3]. This is due to its smaller diameter and the flaccidity of the vessel wall compared to the arteries [4,5]. There also is a risk for postoperative occlusion of the anastomosed vein. Especially when the dorsal veins are severely damaged, and thus, not good candidates for revascularization, the problems could be even more complicated. Furthermore, sometimes surgeons are not inclined to use the dorsal vein as an anastomosed pedicle because the injured part is localized in the volar aspect. Successful fingertip replantation by repairing only the digital artery without venous anastomosis has been reported on occasionally in the literature [6,7]. To maintain outflow from artery-only replants until venous outflow is restored naturally, multiple techniques have been described including periodic puncturing [8]. Given the safety and efficacy of artery-only anastomosis in distal digital replantation, we adopted this approach for reconstruction of the fingertip area with free toe tissue transfer.
Therefore, this study was carried out to evaluate the feasibility of free toe tissue transfer without venous repair in fingertip reconstruction.
METHODS
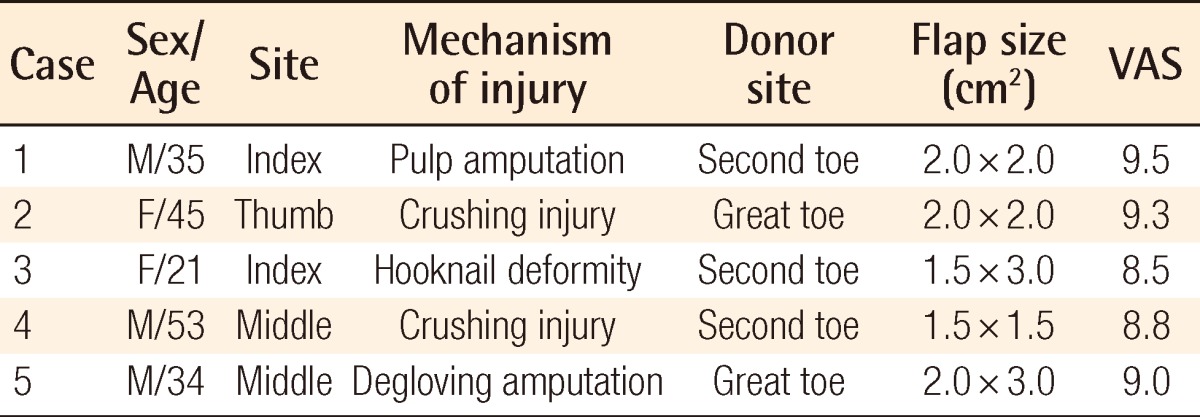
A total of 5 patients were included in the study, consisting of 2 males and 3 females (Table 1). The cases included one thumb, two index fingers, and two middle fingers. All of the patients underwent primary reconstruction after amputation except the case of hook-nail deformity on the index finger. All of the operations were performed under general anesthesia and by the same surgical team. Donor tissues were harvested with the traditional free toe tissue transfer methods. In 2 cases, donor tissue was harvested from the lateral side of the great toes; in the rest, it was harvested from the mediovolar side of the second toes.
The proximal amputated portion was prepared under a surgical microscope, and sufficient arterial bleeding was confirmed before arterial anastomosis. Additional dissection was not necessary at the proximal portion for reconstruction of the amputated finger, but for the hook-nail deformity it was partially performed to release scar contracture simultaneously. With the use of a finger tourniquet, only proper plantar digital arteries were anastomosed using 10-0 nylon sutures. Arterial anastomoses were performed within the wound or within 2 cm proximal to the defect. The digital nerves were repaired to improve sensation and decrease symptoms of neuroma.
Venorrhaphy was not performed in any of the cases; hence no additional incision or dissection for volar vein anastomosis was needed in the harvested flaps or recipient sites. After surgery, the patients were placed in a warm room with a heat lamp, and their hands were elevated above the level of their hearts. The patients were administered 500 mL of low-molecular weight dextran intravenously for 5 consecutive days, but heparin was not used.
Temperature, color, and percutaneous oxygen saturation was monitored and compared with the corresponding contralateral digit to evaluate postoperative venous congestion. Change in flap color or significant flap fullness was regarded as a sign of congestion, and drainage was performed using periodic puncture of the fingertip. Within 24 hours postoperatively, periodic pin-pricking was carried out every 2 hours. After 24 hours, 4-hour intervals were sufficient for venous drainage. Pin-pricking had been continued for 5 days in the case-4-patient, but it was sufficient to relieve venous congestion for 3 days in the other cases.
Moreover, patency of the anastomosed artery was established by monitoring capillary refilling and the Doppler sound. Every patient was informed about the importance of smoking cessation after surgery to prevent poor surgical outcomes.
The functional and cosmetic outcomes were assessed on postoperative follow-ups. The patients' satisfaction was also evaluated using a visual analogue scale, with a score of 0 being the worst and 10 being the best.
RESULTS
Flap sizes ranged from 1.5×1.5 cm2 to 2.0×3.0 cm2, and the mean operation time was 2 hours and 20 minutes. Arterial anastomosis was successful in all 5 patients, and vein grafting for arterial repair was not necessary in any of the cases. None of the cases showed arterial insufficiency or flap loss.
In all the cases, venous congestion was noted in postoperative monitoring, but the patients recovered in 3 to 5 days without secondary procedures except periodic pin-pricking. The amount of blood loss was less than 0.2 mL during each puncture procedure; therefore, blood transfusion was not required in any patients. The mean hospital stay was approximately 10 days.
The mean postoperative follow-up period was 7 months, and significant flap atrophy was not observed. The mean score of patient satisfaction was 9.02±0.40 measured using a visual analogue scale.
Neither pain nor significant sensory loss was observed in any of the cases.
Case 1
A 35-year-old male amputated his right index fingertip. A primarily composite graft was performed, but it failed with necrotic change. Reconstruction was performed with the mediovolar aspect of the left second toe and the tissue survived (Fig. 1).
Case 2
A 45-year-old female had a crushing amputation on her left thumb tip. The amputated tip was well reconstructed using left great toe tissue transfer (Fig. 2).
Case 3
A 21-year-old female had a hook-nail deformity on her right index finger (Fig. 3). Reconstruction using the mediovolar aspect of the left second toe was performed, and the hook-nail deformity was corrected.
DISCUSSION
Fingertip injury is one of the most common hand injuries, and numerous techniques have been attempted to treat it. Healing by primary closure and revision amputation can be the most straightforward method, but they can cause hook-nail deformity or neuroma formation at the stump. Skin grafts are another option, but only for defects without bone or tendon exposure [9]. Various local flaps have been developed to reconstruct fingertips including V-Y flaps, cross-finger flaps, thenar flaps [10], and island flaps [11]. However, postoperative scar contracture or flexion deformity remained as sequelae, and sometimes those flaps are not possible for treating a tip defect such as a transversely amputated stump or pure pulp defect extended to the middle phalanx. Because advances in microsurgery allow options for microsurgical restoration of distal digits, free toe tissue transfer has become the superior choice over conventional techniques in esthetics and function [12].
Adequate venous outflow is one of the most important factors for successful free toe tissue transfer including distal digital reconstruction [3]. Of course it is the safest option if at least one successfully anastomosed vein is present. However, previous studies have provided convincing evidence that amputated fingertips can be salvaged successfully using only arterial anastomosis with simple surgical or nonsurgical methods of venous drainage [13-15]. We adopted this method for free toe tissue transfer for fingertip reconstruction. All 5 of our cases of free toe tissue transfer of artery-only anastomosis survived without significant complications. Periodic pin-pricking did not require blood transfusion or prolonged hospitalization. We believe that this consistent result comes from the wide contact surface between the donor flap and recipient site compared to the flap volume. A wide contact surface enhances early revascularization of a replanted flap, and for that reason total flap survival was achieved.
In some ways our procedure could be considered a form of free composite graft. However, the donor tissue in a composite graft is totally devitalized because there is no blood flow initially. This is the biggest and the most important difference between a composite graft and our procedure. Although survival of a free tissue transfer is critically dependent on the patency of arterial and venous anastomosis in the early phase, the vascular stability of the transferred flap is eventually affected by neovascularization between the donor and recipient tissue. Therefore, vascular development in the contact area is another important factor for flap survival. If the donor tissue has its own vascular supply, this process can be facilitated. Even considering the arterial flow alone, the donor tissue had a vascular component in our cases, and we believe this promoted neovascularization on the contact surface. Furthermore, a harvested donor flap was less limited in size and dimension than a composite graft due to this reliable arterial supply.
Furthermore, toe tissue transfer with the arterial-anastomosis-only technique has some advantages over the conventional anastomosis of both arteries and veins. There is no need for an additional dissection or anastomosis for the veins; thus, simplification of the surgical procedure can be achieved, and the mean operation time would be shortened.
This also helps to reduce the internal damage of a harvested flap. Sometimes a transferred flap requires a smaller and thinner volume of soft tissue for an esthetically pleasing result. As the concerns about supermicrosurgery increase and the techniques continue to be developed, surgical attempts can be made for difficult venous anastomosis in these small flaps. However, dissection for finding venous outflow may cause severe internal injuries. In our method, dissection procedures were simplified to lower the risk of flap damage. Additionally, flaps can have some variations in design because there is no obligation to include veins.
The patient satisfaction results also verified the cosmetically acceptable outcomes. A fingertip is not only functional but also esthetically important for a hand. Because there was no need of additional incisions for the recipient veins, scars were minimized and the patients were satisfied with the results.
There are some disadvantages of arterial-only anastomosis in free toe pulp transfer. Close and frequent observation is needed for early recognition of flap congestion and periodic pin-pricking. It is also difficult to verify the adequate timing and bleeding amount due to the lack of a decongestion guideline. The limitation of this study is related with determining the adequate flap size and volume. We empirically assumed the suitable flap size for artery-only anastomosis, but further studies should be conducted for a general consensus on a maximum flap volume amount to transfer without venous anastomosis.